🚀 From Google Podcasts to Moon FM in No Time: Your Hassle-Free Migration Guide
👉

Cardionerds is a medical cardiology podcast and platform that democratizes cardiovascular education and brings high yield cardiovascular concepts in a fun and engaging format to listeners of all levels.
Join CardioNerds Heart Failure Section Chair Dr. Jenna Skowronski, episode lead Dr. Merna Hussein, and expert faculty Dr. Milton Packer as they discuss the SUMMIT trial.
The SUMMIT trial randomized 731 patients with HFpEF with LVEF ≥ 50% and obesity with BMI ≥ 30 kg/m2 to receive tirzepatide or placebo for at least 52 weeks. The two co-primary endpoints were a composite of time to cardiovascular death or a worsening heart failure event and quality of life measured by the Kansas City Cardiomyopathy Questionnaire clinical summary score (KCCQ-CSS). Treatment with tirzepatide led to a lower risk of the composite of cardiovascular death or worsening heart failure as well as improved quality of life.
This episode was planned in collaboration with the American College of Cardiology Section of the Prevention of Cardiovascular Disease with mentorship from Section Chair Dr. Eugenia Gianos.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Journal Club Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
Packer, M., Zile, M. R., Kramer, C. M., Baum, S. J., Litwin, S. E., Menon, V., Ge, J., Weerakkody, G. J., Ou, Y., Bunck, M. C., Hurt, K. C., Murakami, M., Borlaug, B. A., & SUMMIT Trial Study Group. (2024). Tirzepatide for Heart Failure with Preserved Ejection Fraction and Obesity. The New England Journal of Medicine. https://doi.org/10.1056/NEJMoa2410027
Join CardioNerds Heart Failure Section Chair Dr. Jenna Skowronski, episode lead Dr. Apoorva Gangavelli, and expert faculty Dr. Ronald Witteles as they discuss the Nex-Z trial.
This was a phase 1, open-label trial investigating nex-z, a CRISPR-Cas9-based treatment, in 36 patients with transthyretin amyloidosis with cardiomyopathy (ATTR-CM). The primary objectives were aimed at studying the safety and pharmacodynamics of this novel gene-based treatment modality. This episode dives into the nuances of the data, future directions for investigation, and future clinical implications.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Journal Club Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
Fontana, M., Solomon, S. D., Kachadourian, J., Walsh, L., Rocha, R., Lebwohl, D., Smith, D., Täubel, J., Gane, E. J., Pilebro, B., Adams, D., Razvi, Y., Olbertz, J., Haagensen, A., Zhu, P., Xu, Y., Leung, A., Sonderfan, A., Gutstein, D. E., & Gillmore, J. D. (2024). CRISPR-Cas9 Gene Editing with Nexiguran Ziclumeran for ATTR Cardiomyopathy. The New England Journal of Medicine. https://doi.org/10.1056/NEJMoa2412309
Join CardioNerds co-founder Dr. Daniel Ambinder, episode lead Dr. Nidhi Patel, and expert faculty Dr. Keith Ferdinand as they discuss the BP ROAD trial.
The BP ROAD trial randomized 12,821 patients 50 years of age or older with type 2 diabetes, elevated systolic blood pressure, and an increased risk of cardiovascular disease to receive intensive treatment that targeted a systolic blood pressure of less than 120 mm Hg or standard treatment that targeted a systolic blood pressure of less than 140 mm Hg for up to 5 years. Investigators found a significant reduction of major cardiovascular events with intensive blood pressure lowering. This episode dives into the nuances of the data and clinical implications.
This episode was planned in collaboration with the American College of Cardiology Section of the Prevention of Cardiovascular Disease with mentorship from Section Chair Dr. Eugenia Gianos.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Journal Club Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
Bi, Y., Li, M., Liu, Y., Li, T., Lu, J., Duan, P., Xu, F., Dong, Q., Wang, A., Wang, T., Zheng, R., Chen, Y., Xu, M., Wang, X., Zhang, X., Niu, Y., Kang, Z., Lu, C., Wang, J., … Wang, W. (2024). Intensive Blood-Pressure Control in Patients with Type 2 Diabetes. New England Journal of Medicine. https://doi.org/10.1056/NEJMoa2412006
CardioNerds (Dr. Dan Ambinder and guest host, Dr. Pooja Prasad) join Dr. Donny Mattia from Phoenix Children’s pediatric cardiology fellowship, Dr. Sri Nayak from the Mayo Clinic – Arizona adult cardiology fellowship, and Dr. Harrison VanDolah from the University of Arizona College of Medicine – Phoenix Med/Peds program for a sunrise hike of Piestewa Peak, followed by some coffee at Berdena’s in Old Town Scottsdale (before the bachelorette parties arrive), then finally a stroll through the Phoenix Desert Botanical Gardens to discuss a thought-provoking case series full of clinical cardiology pearls. Expert commentary is provided by Dr. Tabitha Moe. Episode audio was edited by Dan Ambinder.

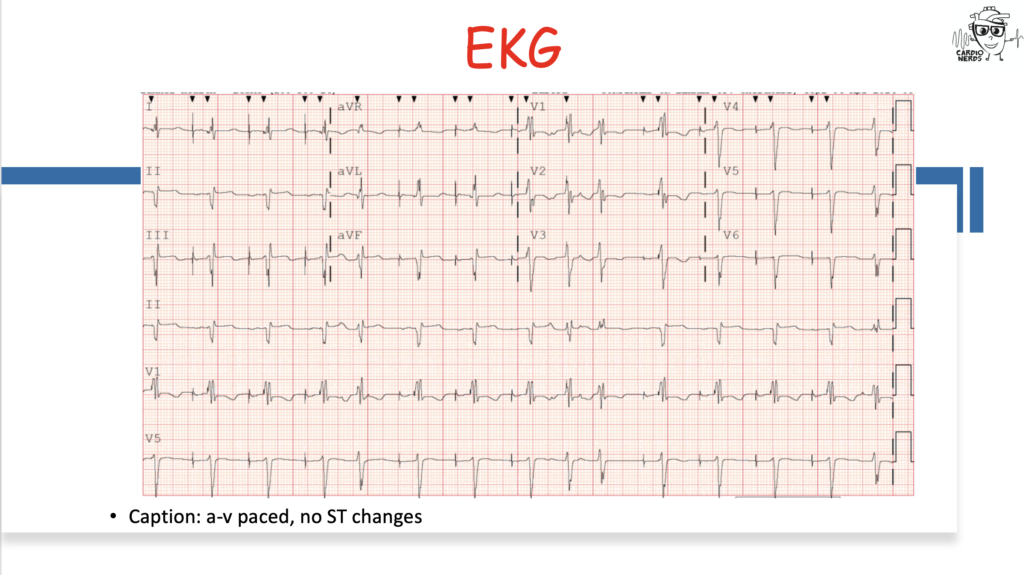
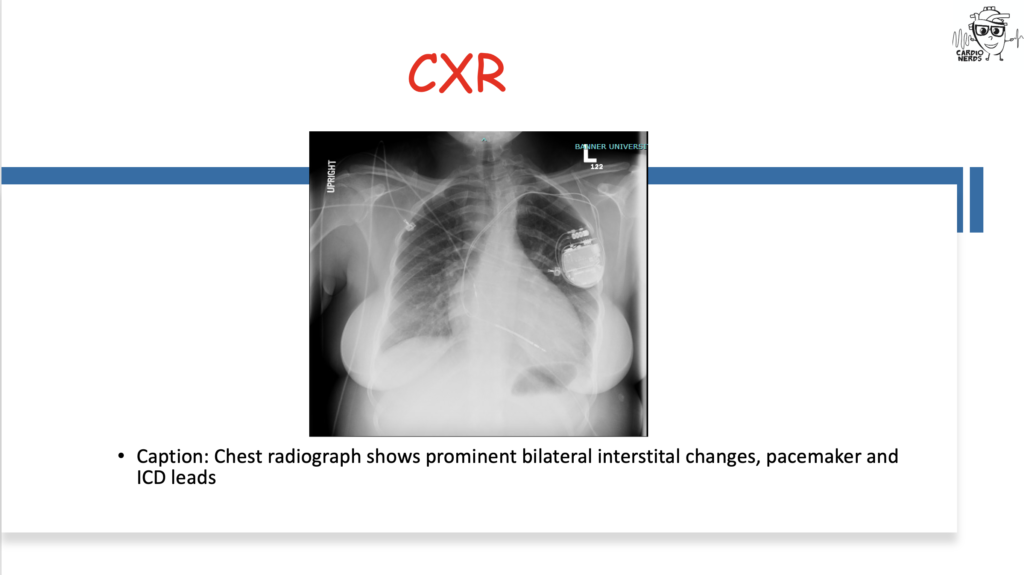
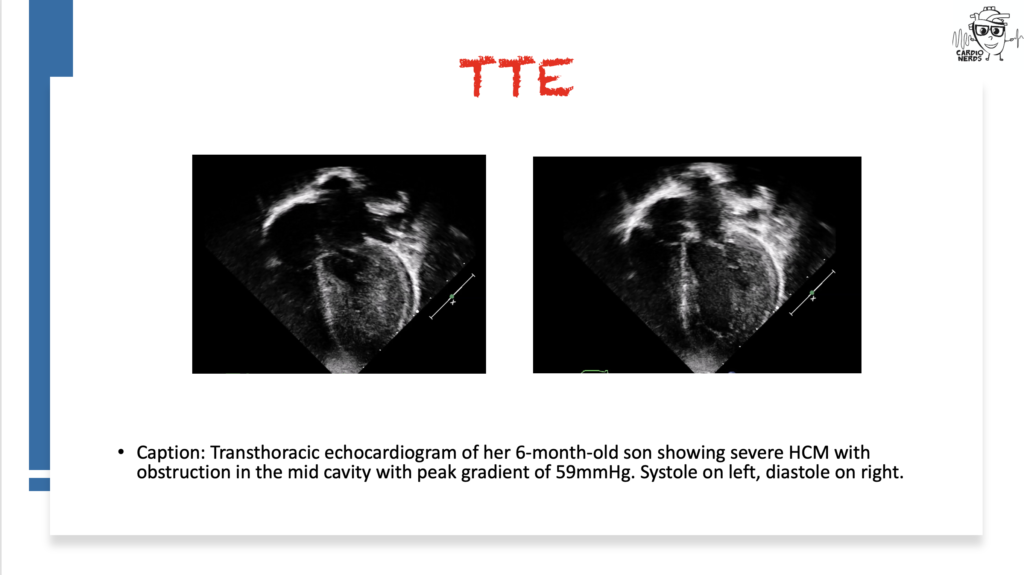
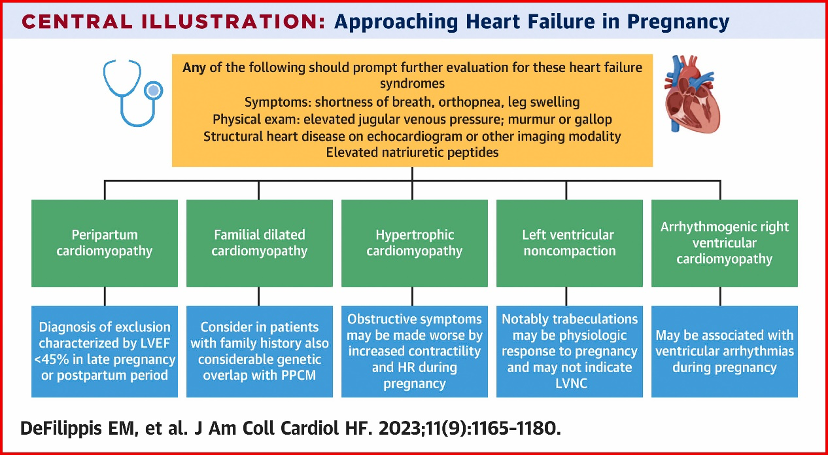
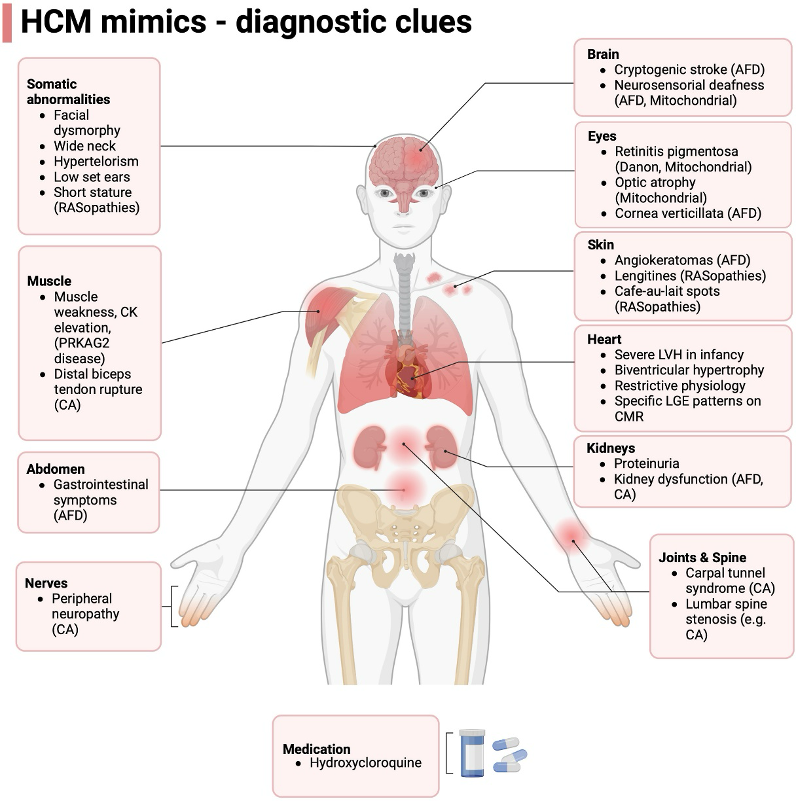
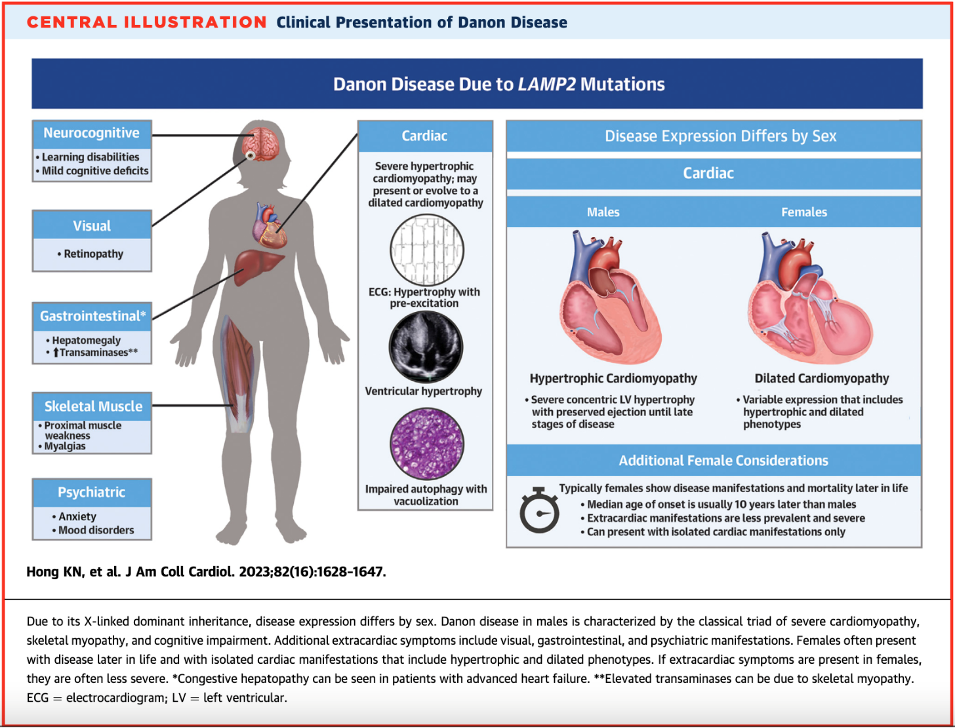
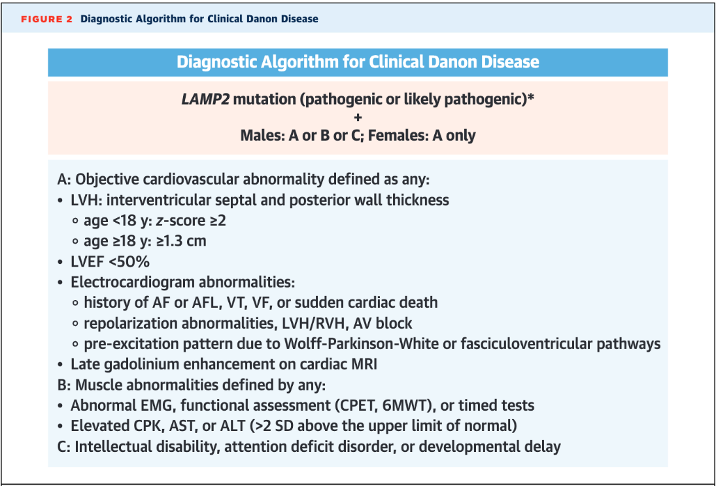
They discuss the following case: Cardiology is consulted by the OB team for a 27-year-old female G1, now P1, who has just delivered a healthy baby boy at 34 weeks gestation after going into premature labor. She is experiencing shortness of breath and is found to have a significant past cardiac history, including atrial fibrillation and preexcitation, now with a pacemaker and intracardiac defibrillator. We review the differential diagnosis for peripartum cardiomyopathy (PPCM) and then combine findings from her infant son, who is seen by our pediatric cardiology colleagues and is found to have severe hypertrophic cardiomyopathy (HCM). Genetic testing for both ultimately reveals a LAMP2 mutation consistent with Danon Disease. The case discussion focuses on the differential diagnosis for PPCM, HCM, pearls on Danon Disease and other HCM “phenocopies,” and the importance of good history.
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” – Sir William Osler. CardioNerds thank the patients and their loved ones whose stories teach us the Art of Medicine and support our Mission to Democratize Cardiovascular Medicine.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Case Reports Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!


CardioNerds (Dr. Dan Ambinder and Dr. Yoav Karpenshif – Chair of the CardioNerds Critical Care Cardiology Council) join Dr. Munim Khan, Dr. Shravani Gangidi, and Dr. Rachel Goodman from Tufts Medical Center’s general cardiology fellowship program for hot pot in China Town in Boston. They discuss a case involving a patient who presented with stress cardiomyopathy leading to cardiogenic shock. Expert commentary is provided by Dr. Michael Faulx from the Cleveland Clinic. Notes were drafted by Dr. Rachel Goodman. Audio editing by Dr. Diane Masket.
A young woman presents with de novo heart-failure cardiogenic shock requiring temporary mechanical circulatory support who is found to have basal variant takotsubo cardiomyopathy. We review the definition and natural history of takotsubo cardiomyopathy, discuss initial evaluation and echocardiographic findings, and review theories regarding pathophysiology of the clinical syndrome. We also highlight complications of takotsubo cardiomyopathy, with a focus on left ventricular outflow obstruction, cardiogenic shock, and arrythmias.
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” – Sir William Osler. CardioNerds thank the patients and their loved ones whose stories teach us the Art of Medicine and support our Mission to Democratize Cardiovascular Medicine.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Case Reports Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
What is Takotsubo Syndrome (TTS)?
What are the echocardiographic findings of takotsubo cardiomyopathy?
Do patients with TTS generally have EKG changes or biomarker elevation?
What are complications of takotsubo cardiomyopathy?
In this episode, CardioNerds Dr. Gurleen Kaur and Dr. Akiva Rosenzveig are joined by Cardio-Rheumatology experts, Dr. Brittany Weber and Dr. Michael Garshick to discuss treating inflammation, delving into the pathophysiology behind the inflammatory hypothesis of atherosclerotic cardiovascular disease and the evolving data on anti-inflammatory therapies for reducing ASCVD risk, with insights on real-world implementation.
Show notes were drafted by. Dr. Akiva Rosenzveig.
This episode was produced in collaboration with the American Society of Preventive Cardiology (ASPC) with independent medical education grant support from Agepha Pharma.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Prevention Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
The following question refers to Sections 7.3.3 and 7.3.6 of the 2022 ACC/AHA/HFSA Guideline for the Management of Heart Failure.
The question is asked by Palisades Medical Center medicine resident & CardioNerds Academy Fellow Dr. Maryam Barkhordarian, answered first by UTSW AHFT Cardiologist & CardioNerds FIT Ambassador Dr. Natalie Tapaskar, and then by expert faculty Dr. Robert Mentz.
Dr. Mentz is associate professor of medicine and section chief for Heart Failure at Duke University, a clinical researcher at the Duke Clinical Research Institute, and editor-in-chief of the Journal of Cardiac Failure. Dr. Mentz has been a mentor for the CardioNerds Clinical Trials Network as lead principal investigator for PARAGLIDE-HF and is a series mentor for this very Decipher the Guidelines Series. For these reasons and many more, he was awarded the Master CardioNerd Award during ACC22.
The Decipher the Guidelines: 2022 AHA / ACC / HFSA Guideline for The Management of Heart Failure series was developed by the CardioNerds and created in collaboration with the American Heart Association and the Heart Failure Society of America. It was created by 30 trainees spanning college through advanced fellowship under the leadership of CardioNerds Cofounders Dr. Amit Goyal and Dr. Dan Ambinder, with mentorship from Dr. Anu Lala, Dr. Robert Mentz, and Dr. Nancy Sweitzer. We thank Dr. Judy Bezanson and Dr. Elliott Antman for tremendous guidance.
Ms. Kay Lotsa is a 48-year-old woman with a history of CKD stage 2 (baseline creatinine ~1.2 mg/dL) & type 2 diabetes mellitus. She has recently noticed progressively reduced exercise tolerance, leg swelling, and trouble lying flat. This prompted a hospital admission with a new diagnosis of decompensated heart failure. A transthoracic echocardiogram reveals LVEF of 35%. Ms. Lotsa is diuresed to euvolemia, and she is started on carvedilol 25mg BID, sacubitril/valsartan 49-51mg BID, and empagliflozin 10mg daily, which she tolerates well. Her eGFR is at her baseline of 55 mL/min/1.73 m2 and serum potassium concentration is 3.9 mEq/L. Your team is anticipating she will be discharged home in the next one to two days and wants to start spironolactone. Which of the following is most important regarding her treatment with mineralocorticoid antagonists?
A
Spironolactone is contraindicated based on her level of renal impairment and should not be started
B
Serum potassium levels and kidney function should be assessed within 1-2 weeks of starting spironolactone
C
Eplerenone confers a higher risk of gynecomastia than does spironolactone
D
The patient will likely not benefit from initiation of spironolactone if her cardiomyopathy is ischemic in origin
Explanation
The correct answer is B – after starting a mineralocorticoid receptor antagonist (MRA), it is important to closely monitor renal function and serum potassium levels.
MRA (also known as aldosterone antagonists or anti-mineralocorticoids) show consistent improvements in all-cause mortality, HF hospitalizations, and SCD across a wide range of patients with HFrEF.
The RALES trial of spironolactone vs. placebo in highly symptomatic HFrEF (LVEF ≤ 35%, NYHA III-IV), trial of eplerenone vs placebo post-MI in patients with LVEF ≤ 40%, and EMPHASIS-HF trial of eplerenone vs placebo in less symptomatic HFrEF (LVEF ≤ 35%, NYHA II) altogether suggest MRAs confer improvements in all-cause mortality, HF hospitalizations, and sudden cardiac death in patients with HFrEF. Importantly, these benefits have been demonstrated across a wide range of HFrEF severity and etiologies, including ischemic cardiomyopathy (Option D).
Therefore, in patients with HFrEF and NYHA class II to IV symptoms, an MRA (spironolactone or eplerenone) is recommended to reduce morbidity and mortality, if eGFR is >30 mL/min/1.73 m2 and serum potassium is <5.0 mEq/L. Careful monitoring of potassium, renal function, and diuretic dosing should be performed at initiation and closely monitored thereafter to minimize risk of hyperkalemia and renal insufficiency (Class 1, LOE A). MRA therapy in this context provides high economic value.
Adverse Effects of MRAs
Both spironolactone and eplerenone are excreted by the kidney and due to their inhibition of aldosterone signaling, reduce potassium excretion in the urine. For these reasons, the initiation of MRAs is contraindicated in patients with eGFR of ≤30 mL/min/1.73m2 or serum potassium levels of ≥5.0 mEq/L. After starting or intensifying MRA therapy, serum potassium levels and renal function should be rechecked at approximately 1 week, at 4 weeks, and every 6 months thereafter, provided clinical stability. Hyperkalemia can increase the risk of ventricular arrhythmias and death. Unfortunately, this often results in de-escalation or discontinuation of RAASi and a subsequent loss of long-term cardiorenal benefits of maximally tolerated GDMT.
The utility of prescribing potassium binders (e.g., patiromer, sodium zirconium cyclosilicate) to improve outcomes by facilitating continuation of Patiromer and sodium zirconium cyclosilicate remove potassium by exchanging cations leading to increased fecal excretion and thereby lowering serum potassium levels. These have been FDA approved for treatment of hyperkalemia for patients receiving RAASi.
Therefore, the use of potassium binders (patiromer, sodium zirconium cyclosilicate) to improve outcomes by facilitating the continuation of RAASi therapy in patients with HF who experience hyperkalemia (serum potassium level ≥5.5 mEq/L) received a Class 2b recommendation (LOE B-R), but overall utility remains uncertain.
In the DIAMOND trial, patients with HFrEF and hyperkalemia were randomized to patiromer vs. control. In the run-in phase, all patients were started on patiromer, and subsequently, RAASi therapy was initiated/optimized. After this, patients were randomized to continue vs stop patiromer. Hard clinical primary endpoints of time to CV death or first CV hospitalization were changed to mean change in serum potassium due to challenges with recruitment related to the COVID-19 pandemic. There was a significant reduction in the mean change of potassium (0.03 mEq/L in the patiromer group vs. 0.13 mEq/L in the control). Additionally, 85% of the patiromer arm was able to be optimized on RAASi.
Aside from hyperkalemia, troublesome side effects of MRAs include gynecomastia and vaginal bleeding. Eplerenone results in lower rates of these side effects than spironolactone given greater specificity for the aldosterone receptor (Option C).
Main Takeaway
Mineralocorticoid receptor antagonists, like spironolactone and eplerenone, reduce all-cause mortality, HF hospitalizations, and sudden cardiac death in a wide range of patients with HFrEF. Monitoring renal function and potassium levels while on MRA therapy is imperative.
Guideline Loc.
Section 7.3.3
Section 7.3.6
Decipher the Guidelines: 2022 Heart Failure Guidelines Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
The following question refers to Sections 7.4 and 7.5 of the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
The question is asked by the Director of the CardioNerds Internship Dr. Akiva Rosenzveig, answered first by Vanderbilt AHFT cardiology fellow Dr. Jenna Skowronski, and then by expert faculty Dr. Randall Starling.
Dr. Starling is Professor of Medicine and an advanced heart failure and transplant cardiologist at the Cleveland Clinic where he was formerly the Section Head of Heart Failure, Vice Chairman of Cardiovascular Medicine, and member of the Cleveland Clinic Board of Governors. Dr. Starling is also Past President of the Heart Failure Society of America in 2018-2019. Dr. Staring was among the earliest CardioNerds faculty guests and has since been a valuable source of mentorship and inspiration. Dr. Starling’s sponsorship and support was instrumental in the origins of the CardioNerds Clinical Trials Program.
The Decipher the Guidelines: 2022 AHA / ACC / HFSA Guideline for The Management of Heart Failure series was developed by the CardioNerds and created in collaboration with the American Heart Association and the Heart Failure Society of America. It was created by 30 trainees spanning college through advanced fellowship under the leadership of CardioNerds Cofounders Dr. Amit Goyal and Dr. Dan Ambinder, with mentorship from Dr. Anu Lala, Dr. Robert Mentz, and Dr. Nancy Sweitzer. We thank Dr. Judy Bezanson and Dr. Elliott Antman for tremendous guidance.
Mrs. M is a 65-year-old woman with non-ischemic dilated cardiomyopathy (LVEF 40%) and moderate to severe mitral regurgitation (MR) presenting for outpatient follow-up. Despite improvement overall, she continues to experience dyspnea on exertion with two flights of stairs and occasional PND. She reports adherence with her medication regimen of sacubitril-valsartan 97-103mg twice daily, metoprolol succinate 200mg daily, spironolactone 25mg daily, empagliflozin 10mg daily, and furosemide 80mg daily. A transthoracic echocardiogram today shows an LVEF of 35%, an LVESD of 60 mm, severe MR with a regurgitant fraction of 60%, and an estimated right ventricular systolic pressure of 40 mmHg. Her EKG shows normal sinus rhythm at 65 bpm and a QRS complex width of 100 ms.
What is the most appropriate recommendation for management of her heart failure?
A
Continue maximally tolerated GDMT; no other changes
B
Refer for cardiac resynchronization therapy (CRT)
C
Refer for transcatheter mitral valve intervention
Explanation
Choice C is correct. The 2020 ACC/AHA Guidelines for the management of patients with valvular heart disease outline specific recommendations.
In patients with chronic severe secondary MR related to LV systolic dysfunction (LVEF <50%) who have persistent symptoms (NYHA class II, III, or IV) while on optimal GDMT for HF (Stage D), M-TEER is reasonable in patients with appropriate anatomy as defined on TEE and with LVEF between 20% and 50%, LVESD ≤70 mm, and pulmonary artery systolic pressure ≤70 mmHg (Class 2a, LOE B-R).
Conversely, mitral valve surgery may have a role in the following contexts:
Choice A is incorrect. GDMT has been shown to improve MR and LV dimensions in patients with HFrEF and secondary MR, and it is a Class 1 recommendation (LOE B-R) to optimize GDMT before any intervention for secondary MR related to LV dysfunction. This includes both medical GDMT and cardiac resynchronization therapy (CRT) where appropriate. Our patient is still having symptoms despite being on the maximally tolerated doses of medical GDMT. This highlights the importance of a multidisciplinary approach to the management of valvular heart disease in patients with HF in accordance with clinical practice guidelines to prevent worsening of HF and adverse clinical outcomes (Class 1, LOE B-R). A cardiologist with expertise in the management of HF is integral in the shared decision-making for valve intervention and should guide optimization of GDMT to ensure that medical options for HF and secondary MR have been effectively applied for an appropriate time-period and exhausted before considering intervention.
Choice B is incorrect. While CRT has been shown to improve MR, LV dimensions, and outcomes in patients with HFrEF and secondary MR in appropriately selected patients, our patient would not be a candidate given that her QRS duration was < 120ms (Class 3: no benefit, LOE B-R).
Main Takeaway
In patients with severe secondary MR and reduced ejection fraction with persistent symptoms despite GDMT, M-TEER is reasonable in patients with appropriate anatomy as defined on TEE and with LVEF between 20% and 50%, LVESD ≤70 mm, and pulmonary artery systolic pressure ≤70 mmHg. Conversely, surgery may be appropriate for some patients. HF ad VHD should be managed in a multidisciplinary fashion.
Guideline Loc.
Sections 7.4-7.5
Figure 10
Also: Section 7.3 from “Otto, C. M., Nishimura, R. A., Bonow, R. O., Carabello, B. A., rwin, J. P., Gentile, F., Jneid, H., Krieger, ric v., Mack, M., McLeod, C., O’Gara, P. T., Rigolin, V. H., Sundt, T. M., Thompson, A., & Toly, C. (2021). 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. In Circulation (Vol. 143, Issue 5, pp. E72–E227). Lippincott Williams and Wilkins. https://doi.org/10.1161/CIR.0000000000000923”
Decipher the Guidelines: 2022 Heart Failure Guidelines Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!

In this episode, Dr. Paul Ridker, a pioneer in the field of cardiovascular inflammation, joins the CardioNerds (Dr. Gurleen Kaur, Dr. Richard Ferraro, and Dr. Nidhi Patel) to discuss the evolving landscape of inflammation as a key factor in cardiovascular risk reduction. The discussion dives into the importance of biomarkers like high-sensitivity C-reactive protein (hs-CRP) in guiding treatment strategies, the insights gleaned from landmark trials like the JUPITER and CANTOS studies, and the future of targeted anti-inflammatory therapies in cardiology.
Show notes were drafted by Dr. Nidhi Patel. Audio editing by CardioNerds academy intern, Grace Qiu.
This episode was produced in collaboration with the American Society of Preventive Cardiology (ASPC) with independent medical education grant support from Lexicon Pharmaceuticals.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Prevention Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
Why is it important to measure both LDL and hs-CRP, and what factors increase hs-CRP?
What data do we have to support measuring hs-CRP?
What are the guidelines and supportive data on using Colchicine?
What are examples of ongoing trials that will shape the future of our anti-inflammatory toolbox?
The following question refers to Section 7.4 of the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
The question is asked by the Director of the CardioNerds Internship Dr. Akiva Rosenzveig, answered first by Vanderbilt AHFT cardiology fellow Dr. Jenna Skowronski, and then by expert faculty Dr. Clyde Yancy.
Dr. Yancy is Professor of Medicine and Medical Social Sciences, Chief of Cardiology, and Vice Dean for Diversity and Inclusion at Northwestern University, and a member of the ACC/AHA Joint Committee on Clinical Practice Guidelines.
The Decipher the Guidelines: 2022 AHA / ACC / HFSA Guideline for The Management of Heart Failure series was developed by the CardioNerds and created in collaboration with the American Heart Association and the Heart Failure Society of America. It was created by 30 trainees spanning college through advanced fellowship under the leadership of CardioNerds Cofounders Dr. Amit Goyal and Dr. Dan Ambinder, with mentorship from Dr. Anu Lala, Dr. Robert Mentz, and Dr. Nancy Sweitzer. We thank Dr. Judy Bezanson and Dr. Elliott Antman for tremendous guidance.
Mr. S is an 80-year-old man with a history of hypertension, type II diabetes mellitus, and hypothyroidism who had an anterior myocardial infarction (MI) treated with a drug-eluting stent to the left anterior descending artery (LAD) 45 days ago. His course was complicated by a new LVEF reduction to 30%, and left bundle branch block (LBBB) with QRS duration of 152 ms in normal sinus rhythm. He reports he is feeling well and is able to enjoy gardening without symptoms, though he experiences dyspnea while walking to his bedroom on the second floor of his house. Repeat TTE shows persistent LVEF of 30% despite initiation of goal-directed medical therapy (GDMT). What is the best next step in his management?
A
Monitor for LVEF improvement for a total of 60 days prior to further intervention
B
Implantation of a dual-chamber ICD
C
Implantation of a CRT-D
D
Continue current management as device implantation is contraindicated given his advanced age
Explanation
Choice C is correct. Implantation of a CRT-D is the best next step.
In patients with nonischemic DCM or ischemic heart disease at least 40 days post-MI with LVEF ≤35% and NYHA class II or III symptoms on chronic GDMT, who have reasonable expectation of meaningful survival for >1 year,
ICD therapy is recommended for primary prevention of SCD to reduce total mortality (Class 1, LOE A). A transvenous ICD provides high economic value in this setting, particularly when a patient’s risk of death from ventricular arrhythmia is deemed high and the risk of nonarrhythmic death is deemed low.
In addition, for patients who have LVEF ≤35%, sinus rhythm, left bundle branch block (LBBB) with a QRS duration ≥150 ms, and NYHA class II, III, or
ambulatory IV symptoms on GDMT, cardiac resynchronization therapy (CRT) is indicated to reduce total mortality, reduce hospitalizations, and improve symptoms and QOL. Cardiac resynchronization provides high economic value in this setting.
Mr. S therefore meets criteria for both ICD and CRT.
Choice A is incorrect. All patients should be on maximally tolerated doses of GDMT prior to consideration of device implantation to allow for assessment of LVEF recovery. Patients who have experienced myocardial infarction should be reassessed 40 days after the event and after achieving maximally tolerated doses of GDMT.
Choice B in incorrect. For patients in sinus rhythm with a LBBB morphology and QRS duration >150 ms with an LVEF ≤35%, there were significant improvements in 6-minute walk test performance, quality of life, NYHA classification, and LVEF after implantation of CRT. Mortality and hospitalizations were also found to be decreased in patients with CRT-P & CRT-D. Overall, CRT has been shown to have high economic value in these patients.
It should be noted that CRT has the most benefit in patients with a wide QRS (>150 ms), LBBB morphology, and LVEF ≤35%, though trials have shown a modest benefit in special populations. CRT has a Class 2a recommendation (LOE B-NR) in patients with LVEF ≤35%, sinus rhythm, and NYHA Class II, III, or ambulatory IV symptoms on GDMT, with either:
a) Non-LBBB pattern with a QRS duration ≥150 ms
b) LBBB with a QRS duration of 120 to 149 ms
Choice D is incorrect. If LVEF remains ≤35% in a patient with a life expectancy >1 year, trials have shown that ICD placement for primary prevention reduces sudden cardiac death and also has a high economic value. There is no indication that this patient has a life expectancy < 1 year.
Main Takeaway
In patients 40 days post-MI on GDMT with an LVEF that remains ≤35%, ICD therapy for primary prevention is appropriate and cost effective. For those additional with a LBBB and QRS >150 ms, CRT-D is also appropriate and cost effective.
Guideline Loc.
Section 7.4
Decipher the Guidelines: 2022 Heart Failure Guidelines Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
Your feedback is valuable to us. Should you encounter any bugs, glitches, lack of functionality or other problems, please email us on [email protected] or join Moon.FM Telegram Group where you can talk directly to the dev team who are happy to answer any queries.
 The Curbsiders Internal Medicine Podcast
The Curbsiders Internal Medicine Podcast
 Eagle's Eye View: Your Weekly CV Update From ACC.org
Eagle's Eye View: Your Weekly CV Update From ACC.org
 Core IM | Internal Medicine Podcast
Core IM | Internal Medicine Podcast
 The Clinical Problem Solvers
The Clinical Problem Solvers
 JACC Podcast
JACC Podcast
 This Week in Cardiology
This Week in Cardiology