🚀 From Google Podcasts to Moon FM in No Time: Your Hassle-Free Migration Guide
👉

Obsgynaecritcare - critical care, anaesthesia and pain medicine in O&G
Hi Everyone,
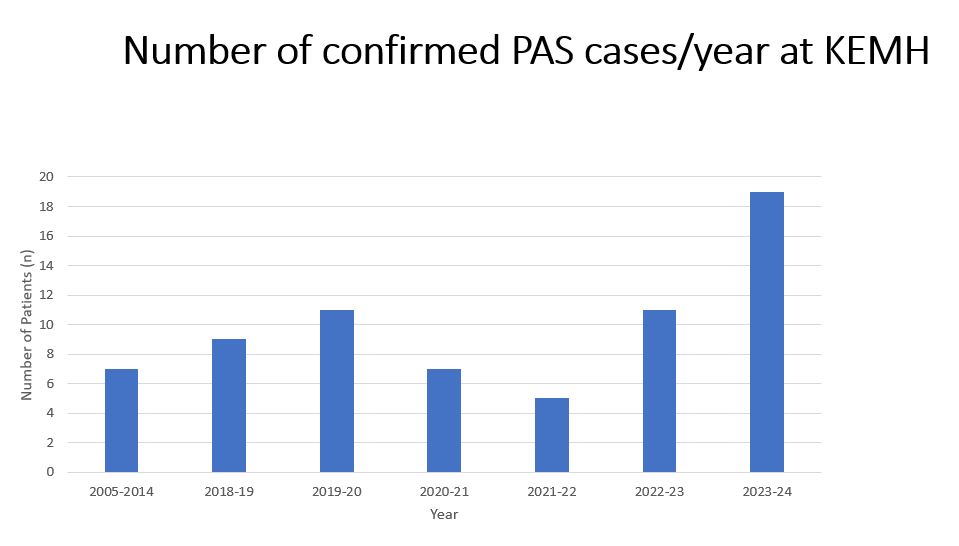
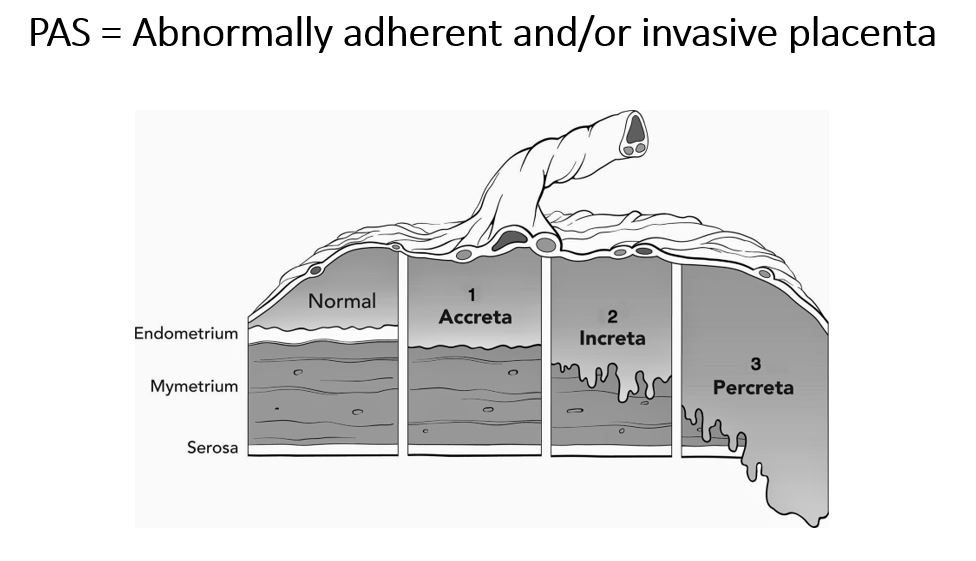
Welcome to Part Two of our discussion with two of the founding members of the Placenta Accreta Spectrum Team here at KEMH Dr Matt Epee-Bekima and Dr David Owen. This team was conceived in 2017 and began operating in 2018 – and has now cared for over 75 women with PAS – including 24 alone this year (2024). In this episode we continue our initial discussion with a more detailed dive into:
Thanks Matt & David for sharing the experiences and knowledge learnt by the PAS team over the last 7 years.

Hi Everyone,
This week I had the privilege of sitting down and recording two fascinating episodes with two of the founding members of the Placenta Accreta Spectrum Team from here at KEMH, Dr Matt Epee-Bekima and Dr David Owen. In this first episode we discuss the following:
King Edward Memorial Hospital website – The Placenta Accreta Spectrum guideline
Hi Everyone,
Join Graeme and I as we discuss two articles chosen from last months edition of IJOA (International Journal of Obstetric Anesthesia). In the first we discuss an article exploring whether the use of intermittent calf compression can reduce hypotension and vasopressor use in women undergoing caesarean section under spinal anaesthesia. The second article looks at the utility of preoperative electrical stimulation of acupressure points prior to caesarean section reduces postoperative pain and improves the quality of maternal recovery. There’s a sprinkling of our usual dad jokes at the end.
For regular listeners to the show join us again later this month when we hopefully will have a couple of episodes dedicated to the management of placenta accreta spectrum and an interview with the founders of the placenta accreta service setup 7 years ago here at KEMH – see you then!
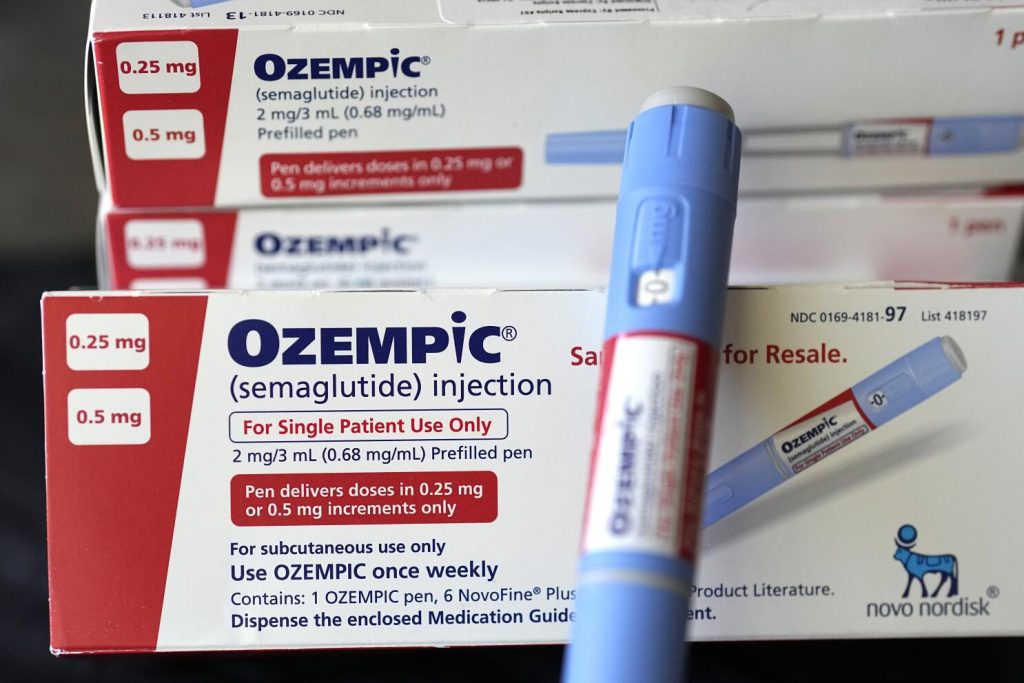
The next patient on your elective list arrives in theatre. She is a 35 year old woman booked for hysteroscopy to investigate her menorrhagia. She has no co-morbidities so wasn’t seen preoperatively in a clinic. She tells you that she has no medical problems but did start on Wegovy for weight loss about 4months ago and has now lost about 12kg. She hasn’t eaten anything since 9pm last night – it is now 10am. You were planning a general anaesthetic and a supra-glottic device, but now you’re not sure what you should do?
Hi everyone,
This week I am joined by Erin and we discuss in detail the perplexing topic of GLP1 receptor agonists. These new wonder weight loss drugs seem to be all the rage and certainly things look rosy if you have shares in Novo Nordisk (the manufacturer). However they are not so great if you provide anaesthesia…. We discuss their relationship with delayed gastric emptying and the risk of aspiration.
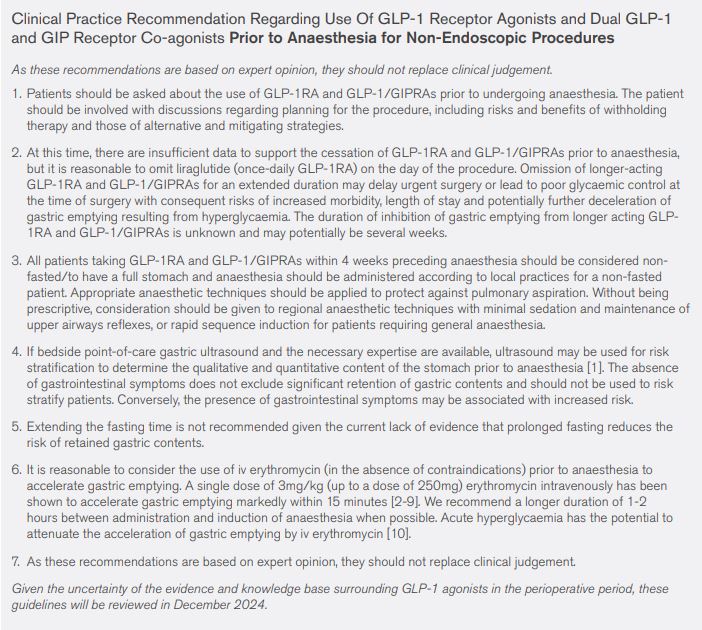
ANZCA GLP1 clinical practice recommendation June 2024
ASA consensus based guidance on preoperative management of GLP1 agonists Feb 2024
Gastricultrasound.org. – This is the best resource available (our humble opinion) if you want to upskill yourself to be able to assess the contents of the stomach.
ANZCA clinical practice recommendation summary – June 2024 see below
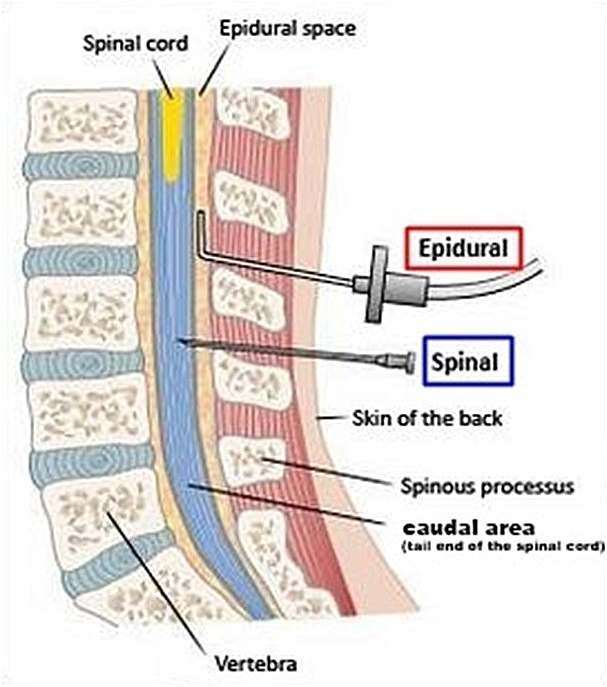
Your patient arrives in the anaesthetic room next to theatre, she’s booked for a non elective caesarean for failure to progress. She has an epidural in situ and you decide try to top it up – however after 25ml of lignocaine 2% with adrenaline and around 20min of waiting the block is stuck at the umbilicus and she can still move her legs relatively freely. This is obviously not going to be adequate – she is adamant she wants to be awake to see her baby born. You sit her up, pull out the epidural and do a single shot spinal with 2.1ml of heavy bupivacaine 0.5% + fentanyl 15mcg – after all you don’t want this block to fail as well!
You clean her back, lie her down and turn to talk to the midwife. When you turn back to the patient 30s later she looks a little purple and isn’t breathing…….
Hi everyone join Graeme and I this week as we discuss total spinal anaesthesia – a fascinating but somewhat scary rare emergency which can occur when we use regional anaesthesia in obstetric practice.
A big shout out to the team from Rotunda Hospital in Dublin who wrote the recent narrative review published in IJOA on this topic!
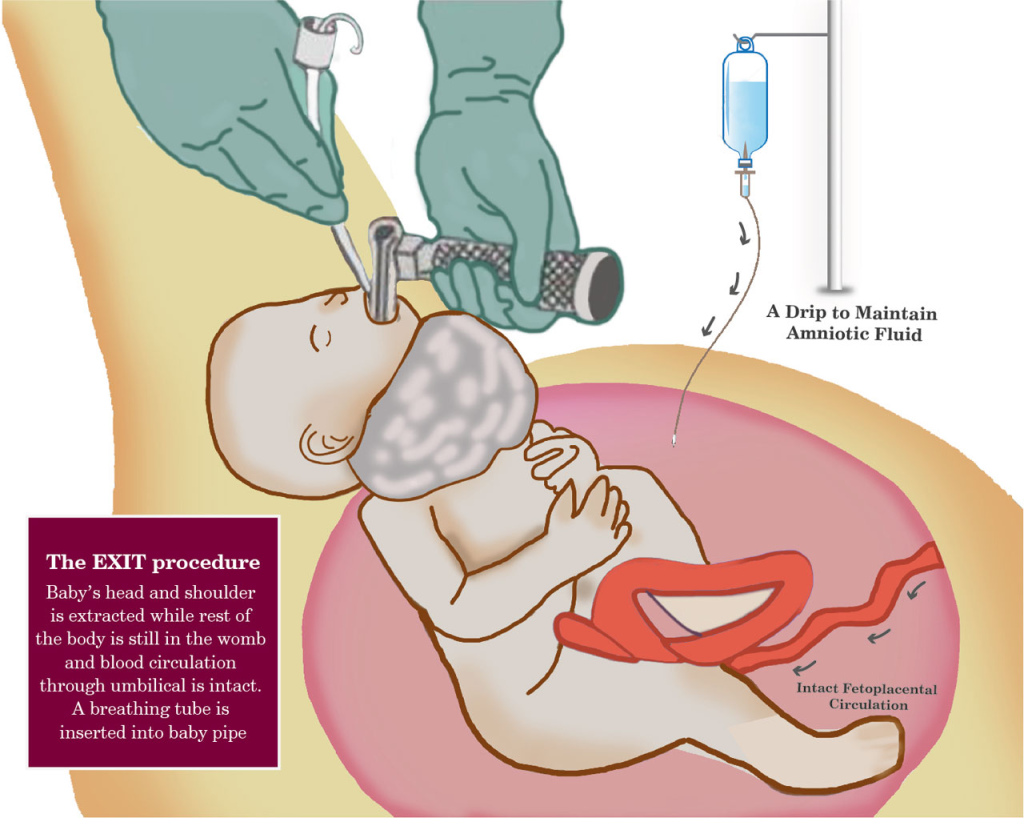
What is the EXIT procedure? Who is it used for and how do we do it?
In our institution this procedure only occurs on average every 3-4 years. It is an event where a large diverse group of individuals, who often have never met each other, come together for a brief period of time to work as a highly complex team to achieve a great result for both the mother and baby.
Join Lloyd and I as we do a deep discussion on this uncommon but challenging multi-disciplinary procedure.
Maternal anesthesia for EXIT procedure: A systematic review of literature.
Hi Everyone,
This week Matt and I agreed to get together to do another journal club episode (or more accurately I printed out an article, put it in Matt’s pigeon hole and told him to make himself available or else!).
We went to one of our favourite journals IJOA (International Journal of Obstetric Anesthesia), where we chose an article from the latest edition published in May.
The article is entitled “A narrative review of the literature relevant to obstetric anesthesiologists: the 2023 Gerard Ostheimer lecture.”
The background to this article is that every year the north american Society of Obstetric Anesthesia and Perinatology (SOAP) hold an annual conference. One of the highlights of these annual conferences is this lecture which is researched and then presented by a well respected obstetric anesthesiologist from the north american community. The lecture is a narrative review of the previous years published literature highlighting important papers and discussing their importance and relevance particularly in relation to current north american practice.
This year’s lecture was presented by Pervez Sultan from Stanford University, and it is drawn from a review of articles published in 2022 from 66 different journals. Over 12 different themes are discussed including (but not limited to) TIVA for GA Caesareans, dexamethasone for post CS analgesia, predicting epidural blood patch success, dural puncture epidurals and a number of other interesting topics.
Join Matt and I as we discuss these and muse over what relevance they may have to our current practice here in Western Australia as well as a couple terrible olympic themed dad jokes to close!
A narrative review of the literature relevant to obstetric anesthesiologists: the 2023 Gerard W. Ostheimer lecture Int J Obstet Anesth 2024 May:58:103973. doi: 10.1016/j.ijoa.2023.103973. Epub 2024 Jan 3.
Hi everyone,
This week I sit down with Jacob one of the provisional fellows in our department and we discuss the findings from the latest UK National Audit Project – NAP7 – which this time investigated Perioperative cardiac arrest.
A woman collapses with abdominal pain in a restaurant & then the initial evaluation in the ED she is diagnosed with suspected ruptured ectopic pregnancy. She is brought straight into your theatre and you perform a rapid sequence induction. You place your video laryngoscope into her mouth and all you see is vomitus and fluid, your yankauer sucker is blocked with food and doing nothing…………
Hi everyone,
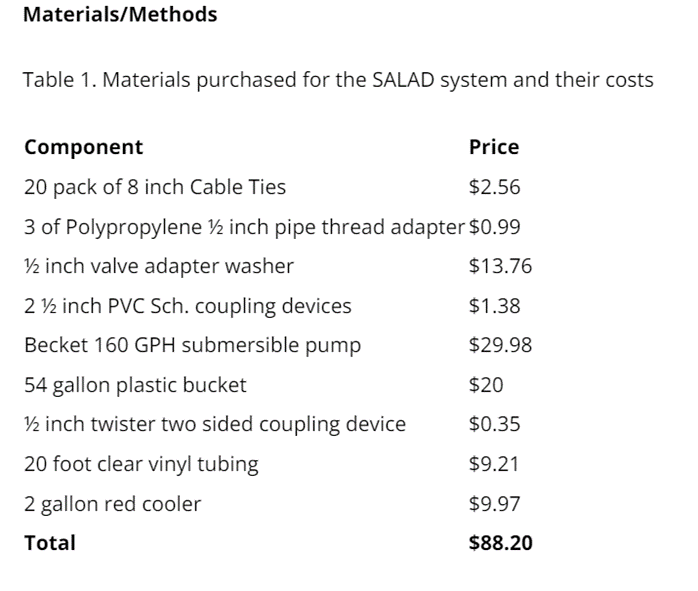
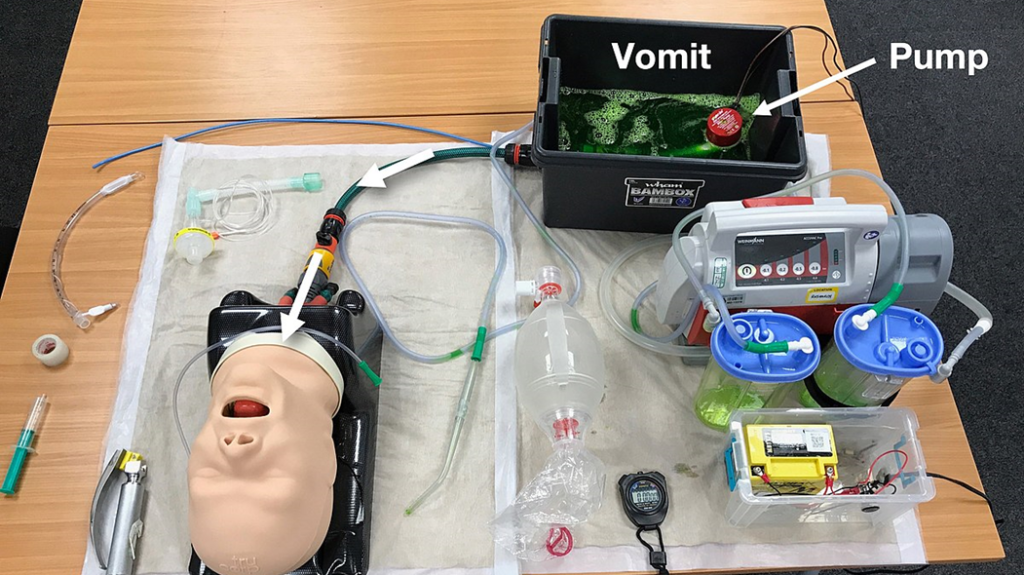
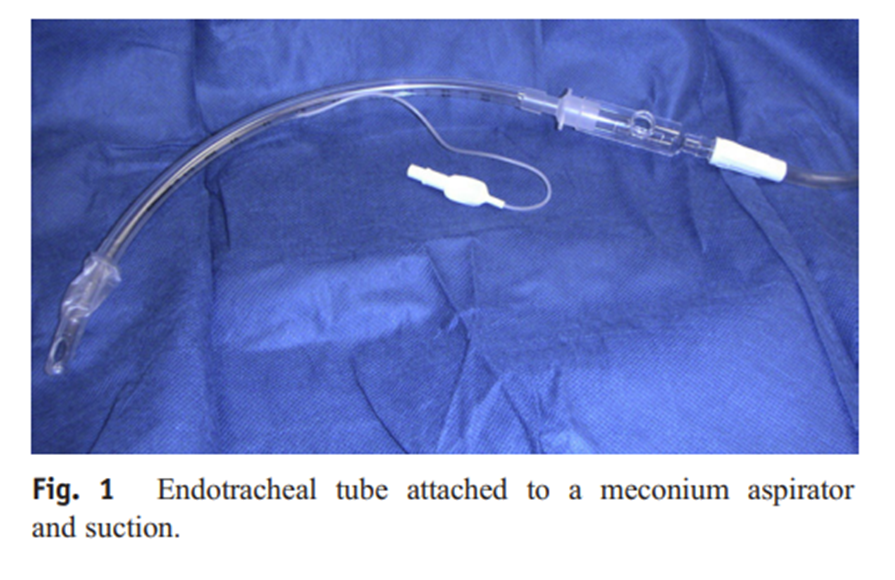
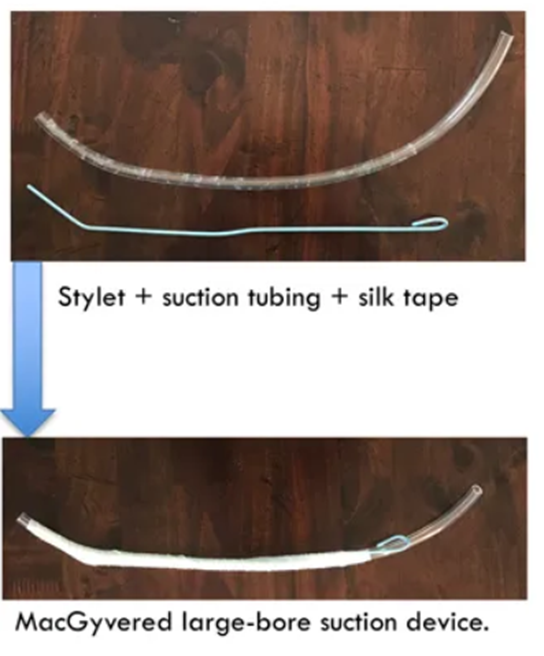
This week I am joined by Dr Nathan Blakely one of our enthusiastic trainees to discuss an area he has taken a personal interest in —- the management of the soiled airway.
Thanks Nathan!
Blood in Airway:


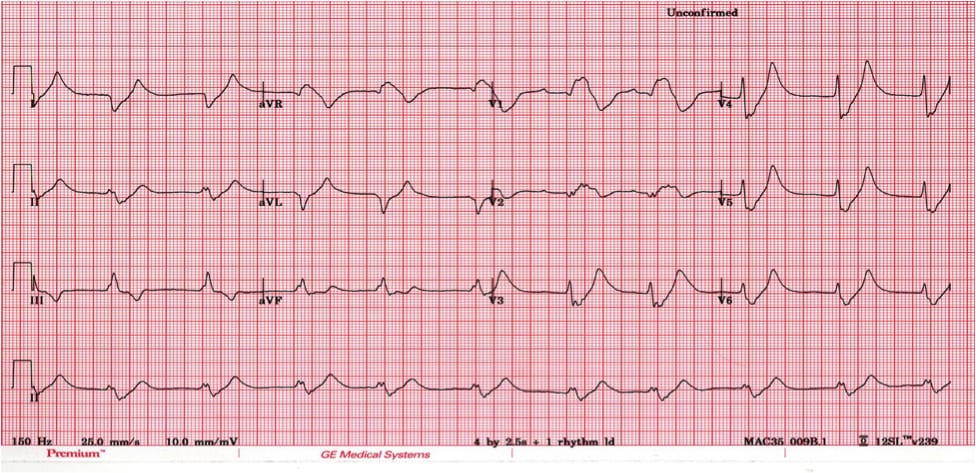
As the DA you are paged to come to PACU to review a patient with pre-eclampsia who has just had a PPH and a repair of a perineal tear after delivering in labour ward. The O&G team ordered a VBG because she was febrile and they want to assess her lactate and start her on some antibiotics. The O&G registrar is concerned however because her potassium / K has come back as 7.8 mmol/L….
Join Natalie and I as we discuss the issue of hyperkalaemia specifically in the context of women suffering from pre-eclampsia. Why are they at risk of this important electrolyte abnormality and what are the principles of management?
We also review a recent paper addressing some of the myths surrounding the treatment of acute hyperkalaemia (thanks to Casey at Broomedocs.com for bringing this paper to our attention).
Gupta AA, Self M, Mueller M, Wardi G, Tainter C. Dispelling myths and misconceptions about the treatment of acute hyperkalemia. Am J Emerg Med. 2022 Feb;52:85-91. doi: 10.1016/j.ajem.2021.11.030. PMID: 34890894
LITFL, ECG library, Hyperkalaemia
https://litfl.com/hyperkalaemia-ecg-libraryA case of probable labetalol induced hyperkalaemia in pre-eclampsia. https://pubmed.ncbi.nlm.nih.gov/25370900
Hypocalcaemia and hyperkalaemia during magnesium infusion therapy in a pre-eclamptic patient https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4614650
Oh’s Intensive Care Manual. 7th Edition. Chapter 93 – Fluid and Electrolyte Therapy. Bersten A, Soni N et al. 2014.
Your feedback is valuable to us. Should you encounter any bugs, glitches, lack of functionality or other problems, please email us on [email protected] or join Moon.FM Telegram Group where you can talk directly to the dev team who are happy to answer any queries.