🚀 From Google Podcasts to Moon FM in No Time: Your Hassle-Free Migration Guide
👉

Rational Evidence Based Evaluation of Literature

 Take Home points:
Take Home points:
Click here for Direct Download of the Podcast.
Definition: a deep laceration that extends into the joint capsule, exposing the intra-articular surface to the environment
Physical Exam:
Diagnostic testing:
ED Management:
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 131.0 – Traumatic Arthrotomy appeared first on REBEL EM - Emergency Medicine Blog.

 Take Home Points
Take Home Points
Click here for Direct Download of the Podcast.
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
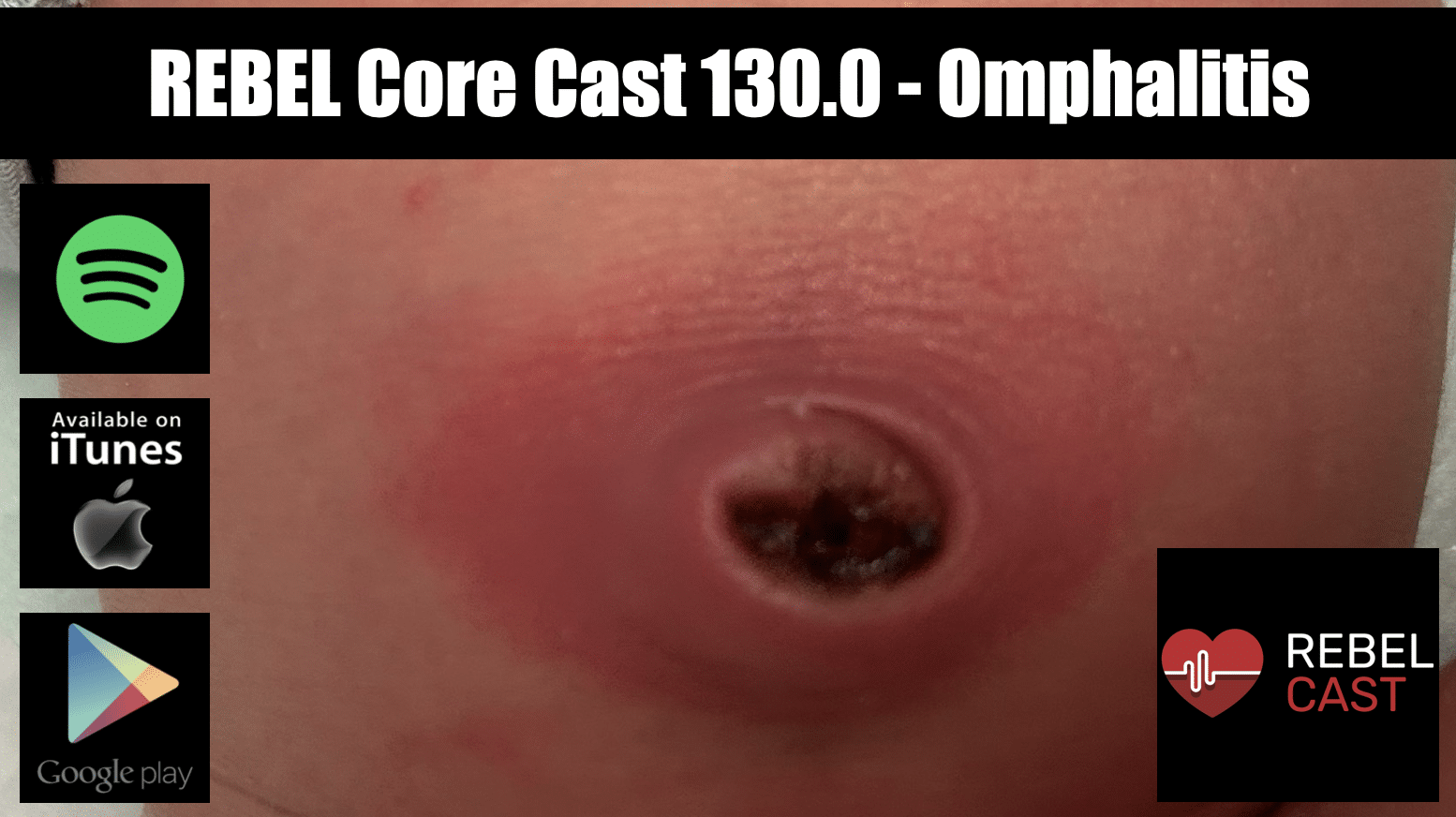
The post REBEL Core Cast 130.0 – Omphalitis appeared first on REBEL EM - Emergency Medicine Blog.

 Take Home Points
Take Home Points
Click here for Direct Download of the Podcast.
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 129.0 – Gastric Lavage appeared first on REBEL EM - Emergency Medicine Blog.

Take Home Points
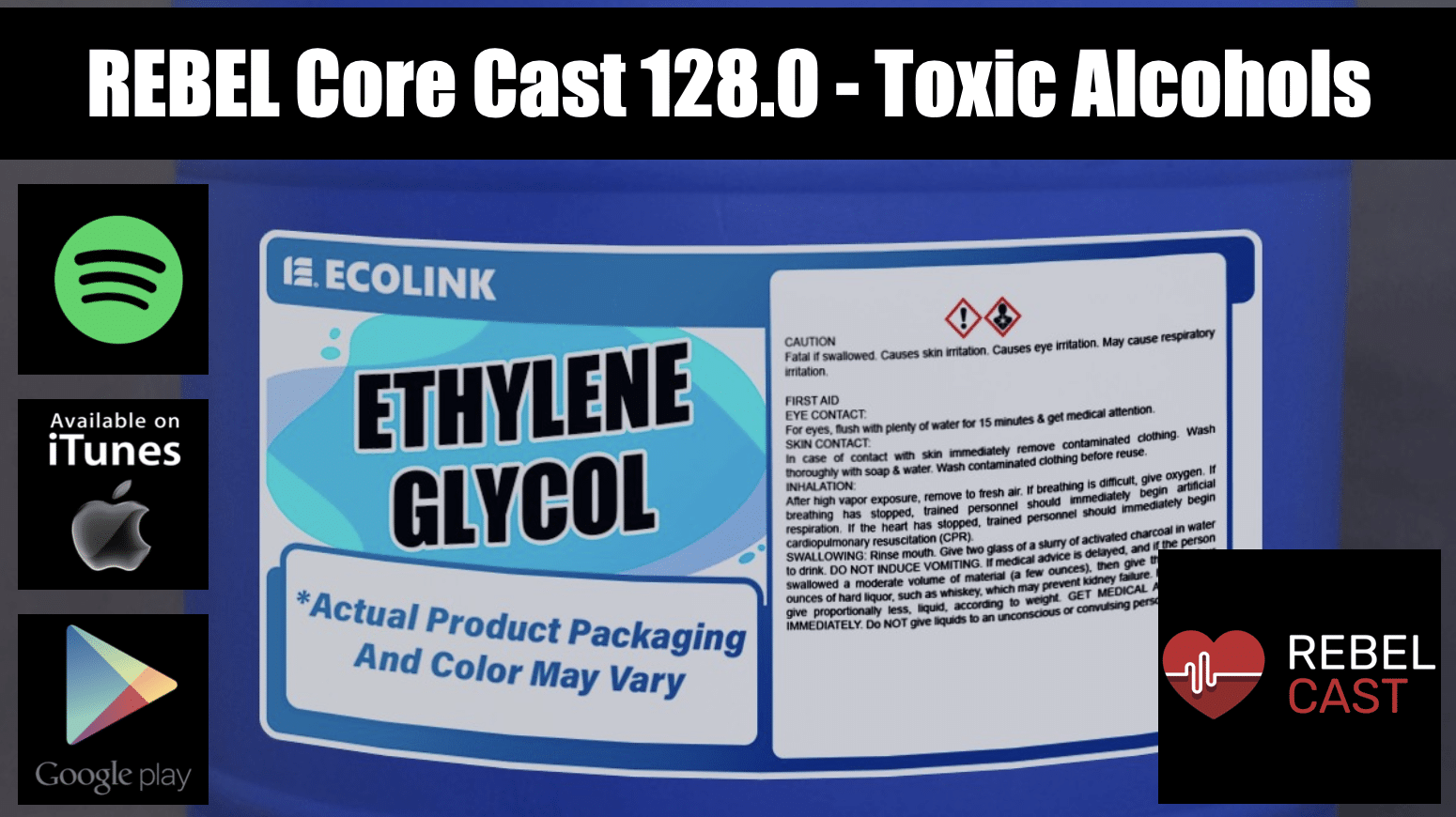 Toxic alcohols generally refer to methanol and ethylene glycol as these substances pose significant metabolic derangement and end-organ damage.
Toxic alcohols generally refer to methanol and ethylene glycol as these substances pose significant metabolic derangement and end-organ damage.
Click here for Direct Download of the Podcast.

Reference: Wiener SW. Chapter 106. Toxic Alcohols. In: Nelson LS, Howland MA, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS, , Flomenbaum NE. eds. Goldfrank’s Toxicologic Emergencies, 11e New York, NY: McGraw-Hill; 2019. Accessed October 2, 2024.
Guest Expert: Dr. Sanjay Mohan, MD (Link)
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 128.0 – Toxic Alcohols appeared first on REBEL EM - Emergency Medicine Blog.

 Take Home Points
Take Home Points
Click here for Direct Download of the Podcast.
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 127.0 – Penetrating Neck Injuries appeared first on REBEL EM - Emergency Medicine Blog.

 Take Home Points
Take Home Points
Click here for Direct Download of the Podcast.
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 126.0 – Peds Hem Onc Emergencies appeared first on REBEL EM - Emergency Medicine Blog.

 Take Home Points
Take Home Points
Click here for Direct Download of the Podcast.
Definition: A serum potassium level > 5.5 mmol/L
Epidemiology
Causes
Clinical Manifestations
Diagnosis
Management
Basics: ABCs, IV, O2, Cardiac Monitor and, 12-lead EKG
Asymptomatic Patients without EKG Changes
Symptomatic Patients or Significant EKG Changes
Asymptomatic Patients with Minor EKG Changes
Take Home Points
References
Elliott MJ et al. Management of patients with acute hyperkalemia. CMAJ 2010; 182(15): 1631-5. PMID: 20855477
Wrenn K et al. The ability of physicians to predict hyperkalemia from the ECG. Ann Emerg Med 1991; 20(11): 1229-32. PMID: 1952310
Aslam S et al. Electrocardiography is unreliable in detecting potentially lethal hyperkalaemia in hemodialysis patients. Nephrol Dial Transplant 2002; 17: 1639-42. PMID: 12198216
Montague BT et al. Retrospective review of the frequency of ECG changes in hyperkalemia. Clin J Am Soc Nephrol 2008; 3:324–330. PMID: 18235147
Mattu A et al. Electrocardiographic manifestations of hyperkalemia. Am J Emerg Med 2000; 18: 721-9. PMID: 11043630
Allon M, Copkney C. Albuterol and insulin for treatment of hyperkalemia in hemodialysis patients. Kidney Int 1990; 38:869–872. PMID: 2266671
Weisberg LS. Management of hyperkalemia. Crit Care Med 2008; 36: 3246-51. PMID: 18936701
Moussavi K et al. Reduced alternative insulin dosing in hyperkalemia: a meta-analysis of effects on hypoglycemia and potassium reduction. Pharmacotherapy 2021; 41(7): 598-607. PMID: 33993515
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 125.0 – Hyperkalemia appeared first on REBEL EM - Emergency Medicine Blog.

 Take Home Points
Take Home Points
Click here for Direct Download of the Podcast.
Background and Physiology
Clinical Manifestations
Traditional Management
HIET
Hyperinsulinemia Euglycemia Therapy (HIET) for BB/CCB Toxicity
References
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 124.0 – Hyperinsulinemia Euglycemia Therapy appeared first on REBEL EM - Emergency Medicine Blog.

 Take Home Points:
Take Home Points:
Click here for Direct Download of the Podcast.
Recognition
Start with the basics
Stopping the Bleeding
Post Placement Care
REBEL EM: Do Patients with Epistaxis Managed by Nasal Packing Require Prophylactic Antibiotics?
REBEL EM: Do Patients with Posterior Epistaxis Managed by Posterior Packs Require ICU Admission?
EMRAP HD: Epistaxis Posterior Pack
References
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 123.0 – Posterior Epistaxis appeared first on REBEL EM - Emergency Medicine Blog.

 Background: In May of 2018, Andexanet alfa gained accelerated approval by the FDA for the reversal direct oral anticoagulants (DOACs) despite a lack of robust evidence for use. The 2022 AHA/ASA guidelines give the drug a level 2A recommendation and recommend it over the use of 4F-PCC (Greenberg 2022). FDA approval alongside guideline endorsement has led to the drug seeing a remarkable growth in use without a single high-quality study to support its use. The available data reports good hemostatic control: a subjective measure that is highly biased by unblinding and selection bias. More importantly, there are no studies comparing andexanet alfa to 4F-PCC or even placebo looking at important, patient-centered outcomes.
Background: In May of 2018, Andexanet alfa gained accelerated approval by the FDA for the reversal direct oral anticoagulants (DOACs) despite a lack of robust evidence for use. The 2022 AHA/ASA guidelines give the drug a level 2A recommendation and recommend it over the use of 4F-PCC (Greenberg 2022). FDA approval alongside guideline endorsement has led to the drug seeing a remarkable growth in use without a single high-quality study to support its use. The available data reports good hemostatic control: a subjective measure that is highly biased by unblinding and selection bias. More importantly, there are no studies comparing andexanet alfa to 4F-PCC or even placebo looking at important, patient-centered outcomes.
Click here for Direct Download of the Podcast.
Article: Connolly SJ et al. Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage (ANNEXA-1). NEJM 2024; 390(19): 1745-55. PMID: 38749032
Clinical Question: Does the use of andexanet alfa in patients on DOACs with intracerebral hemorrhage improved hemostatic efficacy?
Population: Patients > 18 years of age on a factor Xa inhibitor (taken within 15 hours of randomization) with an acute intracerebral hemorrhage.
Outcomes:
Intervention: Andexanet alfa high-dose or low-dose bolus followed by infusion depending on time and dose from last DOAC use.

Control: Usual care
Design: Non-blinded, randomized controlled trial performed at 131 centers across 23 countries over 4 years.
Exclusions
Results:
Critical Results
Andexanet alfa
Usual Care
Difference (95% CI)
P Value
Primary Outcome
Hemostatic Efficacy
67% (150/224)
53.1% (121/228)
13.4 (4.6 – 22.2)
0.003
NIHSS change < 7 points
87.9% (188/214)
83.0% (181/218)
4.6 (-2.0 – 11.2)
Secondary Outcome
Anti-Factor Xa % Change
-94.5% (-96.6 – 88.9)
-26.9% (-54.2 – -9.5)
Safety Outcome
Thrombotic Events
10.3%
5.6%
4.6 (0.1 – 9.2)
0.048
TIA
0
0
Ischemic Stroke
6.5%
1.5%
Myocardial Infarction
4.2%
1.5%
DVT
0.4%
0.7%
PE
0.4%
2.2%
Arterial Embolism
1.1%
0.7%
Death
27.8%
25.5%
0.51
Strengths:
Limitations:
Discussion:
Author Conclusion: “Among patients with intracerebral hemorrhage who were receiving factor Xa inhibitors, andexanet resulted in better control of hematoma expansion than usual care but was associated with thrombotic events, including ischemic stroke.”
Clinical Take Home Point: The authors conclusions are correct. However, they don’t properly stress the findings.
Treatment of patients with intracerebral hemorrhage on a DOAC with Anexanet alfa did not improve clinical outcomes when compared to usual care. Based on safety data, andexanet alfa resulted in increased harm to patients. Andexanet alfa should not be part of the standard treatment in this scenario based on the available evidence.
References:
For More Thoughts on This Topic Checkout:
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post ANNEXA-1: Andexanet Alfa Associated with Harm in DOAC Reversal appeared first on REBEL EM - Emergency Medicine Blog.
 Take Home Points: There are many causes of neutropenia, chemotherapy being by far the most dangerous. Febrile neutropenia is a condition conveying high mortality. Early administration of antibiotics is the only factor known to reduce this mortality. For a patient with neutropenic fever, remember that the body’s own flora is the greatest danger. Isolate, but ... Read more
Take Home Points: There are many causes of neutropenia, chemotherapy being by far the most dangerous. Febrile neutropenia is a condition conveying high mortality. Early administration of antibiotics is the only factor known to reduce this mortality. For a patient with neutropenic fever, remember that the body’s own flora is the greatest danger. Isolate, but ... Read more
The post REBEL Core Cast 122.0 – Neutropenic Fever appeared first on REBEL EM - Emergency Medicine Blog.
Your feedback is valuable to us. Should you encounter any bugs, glitches, lack of functionality or other problems, please email us on [email protected] or join Moon.FM Telegram Group where you can talk directly to the dev team who are happy to answer any queries.
 EM Clerkship
EM Clerkship
 Emergency Medical Minute
Emergency Medical Minute
 The Internet Book of Critical Care Podcast
The Internet Book of Critical Care Podcast
 Critical Care Scenarios
Critical Care Scenarios
 EMCrit FOAM Feed
EMCrit FOAM Feed
 Emergency Medicine Cases
Emergency Medicine Cases