
PulmPEEPs
PulmPEEPs
Pulmonary and Critical Care content for learners and practitioners of all levels
- 1 hour 11 seconds112. Guidelines Series: Pulmonary Hypertension – Definitions, Screening, and Diagnosis
Today we’re kicking off another segment in our Guidelines Series, and doing a deep dive into the 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Over a series of episodes we’ll talk about the most recent updates to definitions around pulmonary hypertension, recognizing and diagnosing Group 1 – 5 pulmonary hypertension, risk stratification, and treatments. In this first episode, we will review the most recent definitions, including changes to the definitions that were new in 2022. We’ll then talk about recognizing and diagnosing pulmonary hypertension with tips and insights along the way.
Meet Our Co-Hosts
Rupali Sood grew up in Las Vegas, Nevada and made her way over to Baltimore for medical school at Johns Hopkins. She then completed her internal medicine residency training at Massachusetts General Hospital before returning back to Johns Hopkins, where she is currently a pulmonary and critical care medicine fellow alongside Tom. Rupali’s interests include interstitial lung disease, particularly as related to oncologic drugs. And she also loves bedside medical education.
Tom Di Vitantonio is originally from New Jersey and attended medical school at Rutgers, New Jersey Medical School in Newark. He then completed his internal medicine residency at Weill Cornell, where he also served as a chief resident. He currently is a pulmonary and critical care medicine fellow at Johns Hopkins, and he’s passionate about caring for critically ill patients, how we approach the management of pulmonary embolism, and also about medical education of trainees to help them be more confident and patient centered in the care they have going forward.
Infographic
Key Learning Points
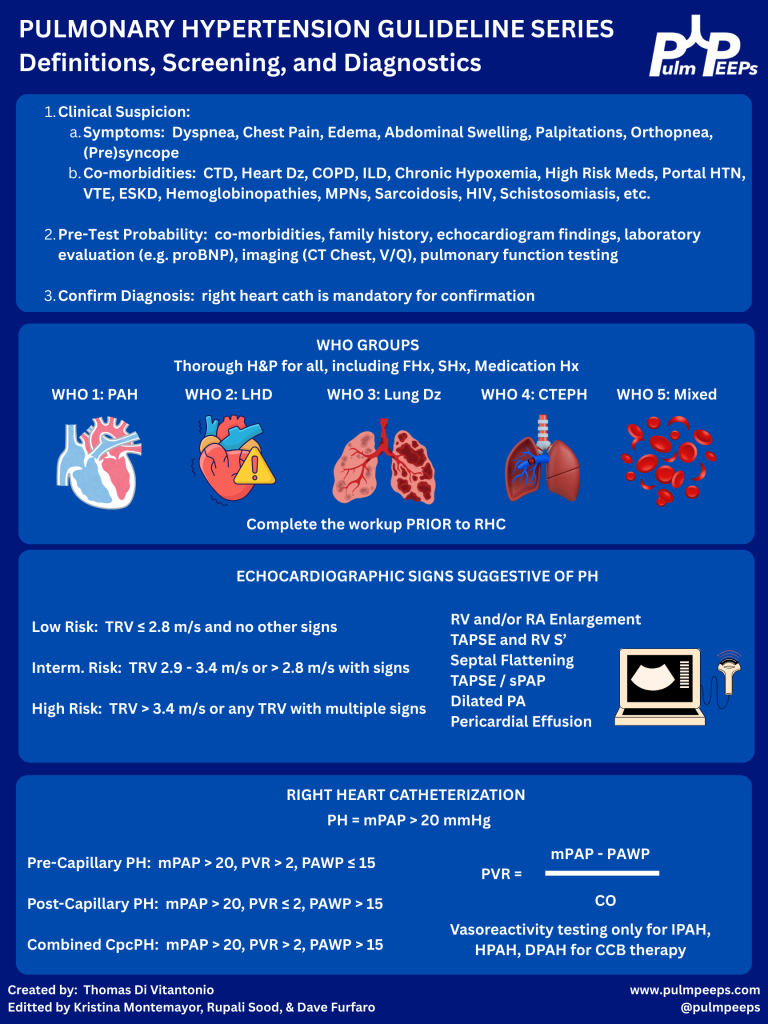
- Why to have a high index of suspicion for pulmonary hypertension (PH)
- PH often presents subtly with slowly progressive dyspnea on exertion, fatigue, lightheadedness, exertional chest pain, or syncope.
- There’s often a delay of 1–2+ years from symptom onset to diagnosis, which is associated with worse mortality.
- Early recognition and treatment, especially for pulmonary arterial hypertension (PAH, WHO group 1), can significantly change outcomes.
- When to suspect PH
Think PH when:
- Dyspnea is out of proportion to:
- CT parenchymal findings (relatively normal lungs)
- Spirometry (normal FEV₁/FVC, volumes)
- There are subtle but progressive symptoms over months:
- Reduced exercise tolerance
- No obvious alternative explanation (e.g., no overt HF, CAD, big ILD, etc.)
- Physical exam may show (often late):
- Elevated JVP, V waves (TR)
- Peripheral edema, hepatomegaly, ascites
- Loud P2, RV heave
In the case: a woman with systemic sclerosis + slowly progressive exertional dyspnea + relatively normal CT parenchyma and spirometry → high suspicion.
- WHO classification: 5 PH groups (big picture + why it matters)
Used for pathophysiology, prognosis, and treatment choices:
- Group 1 – PAH
- Idiopathic, heritable (e.g., BMPR2), drug-induced (e.g., dasatinib)
- Connective tissue disease (esp. systemic sclerosis)
- Portal hypertension (portopulmonary HTN)
- HIV, HHT, congenital heart disease/shunts
- Rare: PVOD, PCH
- Group 2 – PH due to left heart disease
- HFrEF, HFpEF, valvular disease
- Most common cause worldwide.
- Group 3 – PH due to lung disease/hypoxia
- COPD, ILD, combined pulmonary fibrosis–emphysema
- OSA/obesity hypoventilation, chronic hypoxemia
- Group 4 – CTEPH
- Chronic thromboembolic pulmonary hypertension
- Group 5 – Multifactorial/unclear
- Sarcoidosis, myeloproliferative disorders, CKD, sickle cell, etc.
Patients can span multiple groups (e.g., systemic sclerosis: group 1 and/or group 3; sickle cell: many mechanisms).
- Initial workup & refining pre-test probability
Once you suspect PH, you’re trying to answer:
- Does this patient likely have PH?
- If yes, what group(s) are most likely?
Core non-invasive tests:
- NT-proBNP (preferred over BNP)
- Surrogate of RV strain and prognosis.
- Normal value makes significant RV failure less likely.
- Oxygenation & exercise
- Resting SpO₂ plus ambulatory sats; consider 6-minute walk test.
- Exertional desaturation is common and clinically meaningful.
- CXR & ECG
- Low yield but may show RV enlargement, right axis deviation, etc.
- Pulmonary function tests
- Full set: spirometry, volumes, DLCO.
- Clue: isolated or disproportionately low DLCO with relatively preserved FVC suggests pulmonary vascular disease.
- Imaging
- High-res CT chest – parenchymal disease (ILD, emphysema).
- V/Q scan – best screening test for CTEPH; better than CT angiography for chronic disease.
- Sleep testing / overnight oximetry
- When OSA/nocturnal hypoxemia suspected.
- Echo: estimating PH probability (not diagnosis)
TTE is the key screening tool but does not diagnose PH.
Main elements:
- Peak tricuspid regurgitant (TR) velocity
- Used to estimate pulmonary artery systolic pressure (PASP).
- Categories:
- Low probability: TR velocity < 2.8 m/s, no other PH signs.
- Intermediate: 2.9–3.4 m/s ± other PH signs.
- High: > 3.4 m/s.
The presence and severity of TR ≠ TR velocity. You can have severe TR without PH.
- “Other signs” of PH/RV dysfunction on echo:
- RV enlargement or systolic dysfunction (qualitative, TAPSE < ~1.7 cm, S′ ↓)
- RA enlargement
- Septal flattening (D-shaped LV; systolic = pressure overload, diastolic + systolic = volume + pressure)
- Dilated PA
- Pericardial effusion
Interpretation pattern:
- Low pre-test probability + TR v < 2.8 + no other signs → PH unlikely.
- Intermediate TR v (2.9–3.4) + high pre-test probability and/or other PH signs → consider RHC.
- High TR v (>3.4) or clearly abnormal RV → strongly consider RHC if it would change management.
Also:
- Echo is great to follow RV size/function and PASP over time once PH is diagnosed and treated.
Case echo:
- TR velocity 3.1 m/s + mild RA enlargement + moderate RV enlargement + TAPSE 1.6 cm → intermediate probability, consistent with PH and RV involvement.
- Right heart cath (RHC): gold standard & updated definitions
You cannot definitively diagnose or classify PH without RHC.
Key directly measured values:
- RA, RV, PA pressures
- Pulmonary capillary wedge pressure (PCWP/PAWP) ≈ LVEDP
- Oxygen saturations in chambers/vessels
- Cardiac output (thermodilution)
Key derived values:
- Cardiac output (Fick)
- Pulmonary vascular resistance (PVR)
Updated hemodynamic definitions:
- Pulmonary hypertension (PH)
- mPAP ≥ 20 mm Hg (lowered from ≥ 25).
- Pre-capillary PH (think PAH, group 1; also groups 3, 4, some 5):
- mPAP ≥ 20
- PAWP ≤ 15
- PVR > 2 Wood units (new lower threshold)
- Isolated post-capillary PH (IpcPH) (group 2)
- mPAP ≥ 20
- PAWP > 15
- PVR ≤ 2
- Combined pre- and post-capillary PH (CpcPH)
- mPAP ≥ 20
- PAWP > 15
- PVR > 2
Rationale for the changes:
- Normal mPAP in healthy people is < ~19; 20 is about 2 SD above normal.
- Patients with mPAP 20–24 (esp. systemic sclerosis) already have worse outcomes than those < 20.
- Lowering PVR cutoff from 3 → 2 WU better aligns with these new thresholds and catches earlier precapillary disease.
Practical interpretation:
- You use mPAP + PAWP + PVR to:
- Confirm PH.
- Distinguish pre- vs post-capillary.
- Identify mixed disease.
- Echo tells you probability; RHC tells you what type and how severe.
- Vasoreactivity testing (acute vasodilator testing)
- Only indicated in:
- Idiopathic (IPAH)
- Heritable PAH
- Drug-induced PAH
→ Not routine for all PH patients.
- Performed in the cath lab with short-acting vasodilator (e.g., inhaled NO).
Positive test:
- ↓ mPAP ≥ 10 mm Hg
- To an absolute mPAP ≤ 40 mm Hg
- No fall in cardiac output
Why it matters:
- Identifies a small subset who can be treated with high-dose calcium channel blockers long-term and often have better prognosis.
- Does not predict response to other PAH therapies (ERA, PDE5i, prostacyclin, etc.).
- Screening high-risk populations
Some groups warrant systematic screening because of high PAH risk.
- a) Systemic sclerosis / systemic sclerosis spectrum
- Annual screening if:
- Disease duration ≥ 3 years
- FVC ≥ 40% predicted
- DLCO < 60% predicted
- DETECT algorithm (2-step):
- Step 1: uses labs and simple tests (FVC/DLCO ratio, NT-proBNP, autoantibodies, right axis deviation on ECG, telangiectasias).
- If positive → Step 2: adds echo (TR velocity, RA size).
- If high risk after Step 2 → RHC.
- Goal: catch early PAH before symptoms are severe.
- b) Other high-risk groups
Annual screening (usually with echo ± NT-proBNP, PFTs) for:
- Known heritable PAH mutations (e.g., BMPR2)
- Portal hypertension (esp. considering liver transplant or TIPS)
- HIV
Always layer this on top of clinical symptoms and progression.
- Big practical takeaways (what to apply on Monday)
- Don’t label “pulmonary hypertension” off CT or echo alone.
- Enlarged PA on CT or elevated PASP on echo ≠ diagnosis.
- RHC is required.
- Think PH early when:
- Dyspnea is out of proportion to imaging and spirometry.
- There is a relevant risk factor (systemic sclerosis, portal HTN, HIV, prior PE, congenital heart disease, etc.).
- Use the WHO groups to structure your differential and workup:
- Group 1 vs 2 vs 3 vs 4 vs 5 → drives what tests you order and what treatments you eventually consider.
- Echo = probability. RHC = truth.
- Echo gives you low / intermediate / high PH probability.
- RHC gives you pre- vs post-capillary, PVR, and hemodynamics needed for therapy.
- Know the new numbers:
- mPAP ≥ 20 = PH
- PAWP cutoff = 15
- PVR > 2 WU = precapillary component
- Don’t forget NT-proBNP, DLCO, V/Q scan, and high-risk screening (especially in systemic sclerosis and BMPR2 carriers).
References
9 December 2025, 5:15 am - 7 minutes 53 seconds111. Pulm PEEPs Pearls: Methylene Blue
Furf and Monty are back today with another Pulm PEEPs Pearls episode, and discussing the use of methylene blue for patients with septic shock. They review the clinical scenarios when this comes up, the mechanism, some key data, and some take aways, all in 15 minutes! Let us know any other topics you’d like covered on the show and make sure to like, give us 5 stars, and subscribe wherever you’re listening to this podcast.
This episode was prepared in conjunction with George Doumat MD. Goerge is an internal medicine resident at UT Southwestern and joined us for a Pulm PEEPs – BMJ Thorax journal club episode. He is now acting as a Pulm PEEPs Associate Editor for the Pulm PEEPs Pearls series.
Key Learning Points
- Clinical context: when does methylene blue even come up?
- This is not a first-line sepsis drug.
- It’s considered in catecholamine-refractory vasoplegic septic shock, typically when:
- Norepinephrine is at high dose
- Vasopressin is on board
- Often a 3rd or 4th vasopressor is being used (e.g., phenylephrine, angiotensin II)
- The phenotype is strongly vasodilatory/vasoplegic (warm, distributive shock) rather than primarily cardiogenic.
- Mechanism of action (why it might help)
- Methylene blue:
- Inhibits inducible nitric oxide synthase and guanylate cyclase.
- Blunts excess nitric oxide and cyclic GMP–mediated vasodilation, which are key in vasoplegic sepsis.
- Practical translation:
- It restores vascular tone and can make the vasculature more responsive to catecholamines.
- It’s also used in post-CPB vasoplegia (e.g., after cardiac surgery, especially in patients on ACE inhibitors) and has migrated from that world into ICU sepsis practice.
- Typical dosing strategy (as described in the episode)
- Common approach:
- 1–3 mg/kg IV bolus, then
- Reassess hemodynamics (MAP, dynamic perfusion markers).
- If there’s a response, consider a continuous infusion or repeat bolus.
- Key nuance: unlike other pressors that start as drips, methylene blue is often trialed as a bolus first to see if it’s doing anything.
- What does the evidence suggest?
Most data are from small, single-center, heterogeneous studies, so evidence quality is low. Meta-analyses and systematic reviews (through ~2024–25) suggest:
- Hemodynamics
- Can increase MAP (roughly 1–10 mmHg across studies).
- May shorten total vasopressor duration (one meta-analysis ~30 hours less, though this is not definitive).
- Secondary physiologic effects
- Some small improvements in PaO₂/FiO₂ (P/F) ratio in certain studies.
- Clinical outcomes
- Possible reduction in hospital length of stay (≈ up to 2 days in some pooled analyses).
- Some signal toward lower short-term mortality, but:
- Studies are small
- Heterogeneous
- Evidence is very low certainty
- Bottom line:
- There’s a repeatable signal that methylene blue:
- Raises MAP
- Helps reduce catecholamine requirements
- But hard clinical outcomes (mortality, LOS, ventilator days) remain uncertain.
- There’s a repeatable signal that methylene blue:
- Safety profile & important adverse effects
Things to watch for:
- Methemoglobinemia
- Serotonin syndrome
- Especially in patients on SSRIs, though in life-threatening refractory shock the hosts still lean toward using it with caution.
- Pulse oximeter artifact
- Can distort SpO₂ readings.
- Urine discoloration
- Blue/green urine—benign but striking.
Notably:
- Methylene blue is both a treatment for and a potential cause of methemoglobinemia, depending on context and dosing.
- Guidelines & where it fits in practice
- Surviving Sepsis Campaign 2021:
- Does not recommend methylene blue for routine use in septic shock.
- No major critical care society includes it in standard septic shock bundles or protocols.
- The hosts frame methylene blue as:
- A rescue therapy, not guideline therapy.
- Something to consider only in refractory vasoplegic shock, ideally with:
- Multidisciplinary discussion (intensivist, pharmacist, etc.).
- Clear documentation that this is off-guideline, salvage use.
- Practical bedside framing (“2 a.m. in the ICU”)
They emphasize three pillars of practice:
- Physiology – mechanism makes sense (NO / cGMP / vasodilation).
- Empiric evidence – small studies and meta-analyses show a signal but low-quality data.
- Bedside reality – at 2 a.m., with a patient in multi-pressor, refractory vasoplegic shock, you sometimes reach for imperfect tools.
So, the practical take:
- You should NOT:
- Use methylene blue early.
- Treat it as part of standard sepsis care.
- You may consider it when:
- Shock is clearly vasoplegic and refractory.
- Norepi + vasopressin + at least one more vasopressor are maxed.
- Team agrees this is salvage therapy and understands the limited evidence and side effects.
25 November 2025, 5:30 am - 30 minutes 11 seconds110. Pulm PEEPs at CHEST 2025 – Widened Airways and Narrowed Differentials
For today’s podcast we have a special episode. We were extremely grateful to be invited to present live at CHEST 2025 this year. Kristina Montemayor, and Pulm PEEPs Associate Editors Luke Hedrick, Tom Di Vitantonio, and Rupali Sood hosted a session entitled “Widened Airways and Narrowed Differentials”. It is a great session around bronchiectasis. Enjoy!

Meet Our Guests
Dr. Doreen Addrizzo-Harris is a Professor of Medicine at NYU where she is also Associate Director of Clinical and Academic Affairs for the pulmonary and critical care division. In addition to that, she’s the director of the bronchiectasis and NTM program and also serves as a program director for the pulmonary and critical care fellowship.
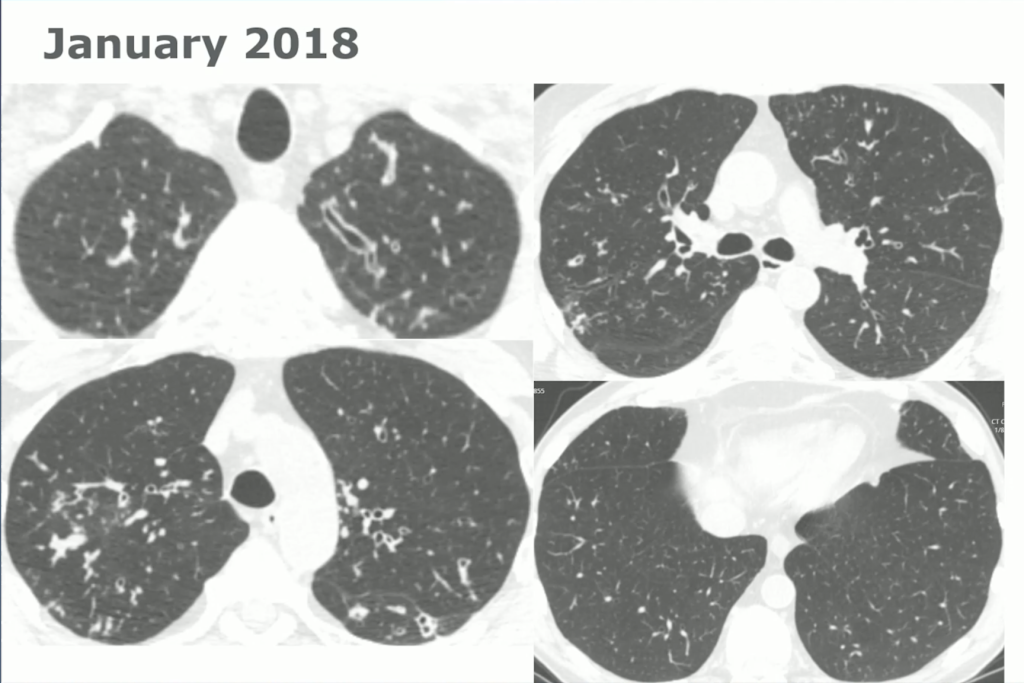
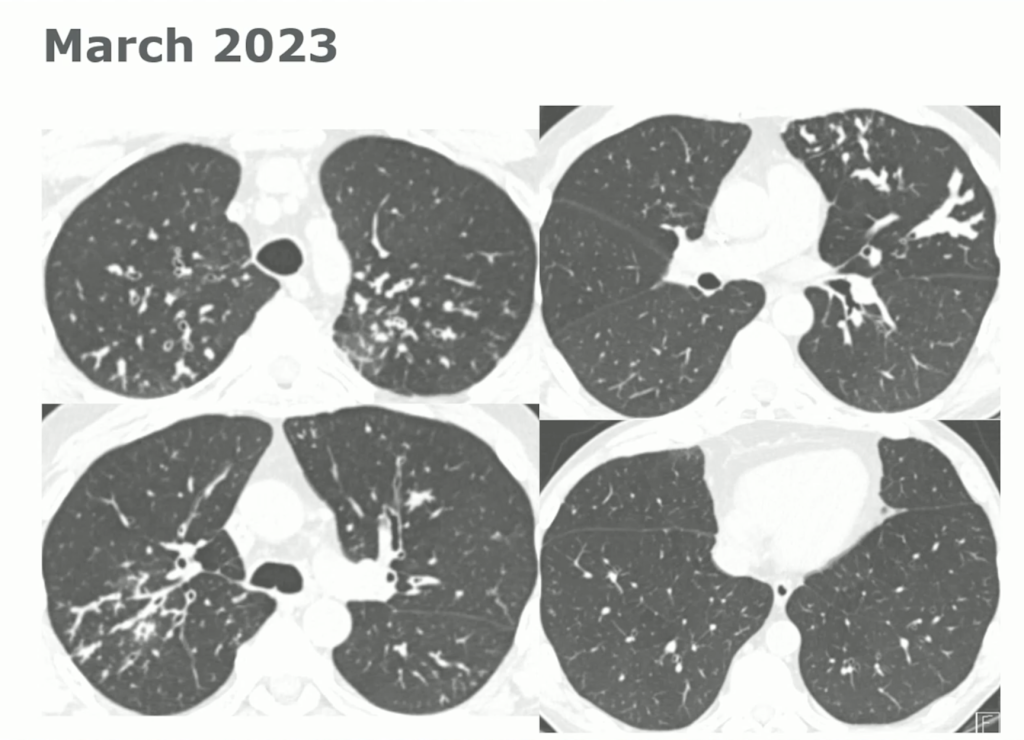
Case Snapshot
60-year-old with CLL (in remission) → recurrent “pneumonias,” diffuse (not single-lobe), later dx’d with CVID; serial CTs: upper-lobe–predominant bronchiectasis, tree-in-bud, mucus impaction; multiple AFB+ cultures (MAC, later M. abscessus); recurrent bacterial flares (MSSA/MRSA).
CT Images

Key Learning Points
Imaging pearls
- Tree-in-bud = small airways (bronchiolar) impaction/inflammation, not a diagnosis. Differential guided by distribution + chronicity:
- Acute/diffuse → bacterial/viral/NTM infection
- Dependent/basal → aspiration
- Persistent + nodular + bronchiectasis → NTM common
- Bronchiectasis CT signs (think: “ring, taper, edge”):
- Broncho-arterial ratio >1 (signet-ring)
- Lack of normal tapering
- Visible bronchi within 1 cm of pleura
- Location matters:
- Upper lobes → CF, sarcoid, prior TB/radiation
- Middle lobe/lingula → NTM classic; consider ABPA if central
- Lower lobes → aspiration, PCD, CTD, immunodeficiency
NTM: diagnosis & when to treat
- Use all three (2020 guideline frame): clinical symptoms, compatible CT, microbiology (≥2 sputum cultures or 1 bronch +, etc.).
- Not every positive culture = disease needing drugs. If you defer pharmacologic therapy, follow closely (symptoms, sputum, PFTs, interval CT if change).
- Bug matters: MAC, M. abscessus, kansasii etc. “Low-virulence” species (e.g., M. gordonae) can still flag underlying airway disease.
- Regimens (MAC, macrolide-susceptible): azithro + ethambutol + rifampin (intermittent for nodular-bronchiectatic; daily ± IV amikacin for fibro-cavitary/advanced).
- Macrolide is the backbone; the others protect against resistance.
- M. abscessus: check for inducible macrolide resistance (prolonged in-vitro testing).
- Monitoring: sputum q1–3 mo; labs (CBC/CMP), vision (ethambutol), hearing (aminoglycosides). Treat ~12 months beyond culture conversion.
- Anti-inflammatory macrolide for bronchiectasis is contraindicated if macrolide-susceptible NTM is present—risk of resistance.
Bronchiectasis management essentials
- It’s a syndrome: symptoms/exacerbations plus CT changes.
- Airway clearance is foundational (exercise + devices ± hypertonic saline/DNase when indicated). Expect CT and symptom gains with adherence.
- Exacerbations often need ~14 days of pathogen-directed antibiotics (short courses may fail). Take the “easy win” when a conventional pathogen explains the flare.
Workup framework (start with a core bundle, then target)
Core “every patient” bundle
- CBC with diff (look for eosinophilia/hematologic clues)
- Quantitative IgG/IgA/IgM (primary/secondary immunodeficiency)
- ABPA screen: total IgE + Aspergillus-specific IgE/IgG
- Sputum cultures: routine bacteria + AFB + fungal (if producing)
- Baseline PFTs
Targeted tests (guided by history, distribution, microbes)
- CF evaluation: sweat chloride and/or CFTR genotyping (especially with upper-lobe disease, chronic sinusitis/nasal polyps, pancreatitis/malabsorption, infertility/CAVD).
- PCD: nasal NO, genetics, specialized ciliary studies (adult cases may be mild and missed by genetics alone).
- Alpha-1 antitrypsin (never-smoker emphysema, liver hx)
- CTD serologies (RA, Sjögren’s, etc.), if suggestive
- Aspiration/upper-GI assessment when basal-predominant or reflux symptoms
- For suspected/known CVID: vaccine response assessment if not on replacement (this patient was already on IVIG).
Practical diagnostic habits
- Re-read the CT yourself—radiology may under-call mild bronchiectasis in ED/PE-protocol scans.
- Use a diagnostic time-out when the course isn’t fitting: name your working dx, list fits/mismatches, consider common diseases with atypical presentations, multi-morbidity, and can’t-miss alternatives; ask for help early; communicate uncertainty.
Teach-to-remember pearls from the case
- Recurrent, geographically scattered pneumonias → think systemic causes (immunodeficiency, CF/PCD), not just focal anatomic problems.
- Upper-lobe bronchiectasis + CAVD is a CF red flag—even in the 60s. Adult-onset CF is real and actionable.
- In CF today, MSSA can be more common than Pseudomonas on culture; don’t let absence of Pseudomonas dissuade you.
- Airway clearance adherence can change CTs; instruct patients to ramp up before surveillance scans for a fair assessment.
- If symptoms abate with targeted therapy to a conventional pathogen, you may avoid immediate NTM re-treatment—but keep a tight follow-up loop.
11 November 2025, 5:15 am - Tree-in-bud = small airways (bronchiolar) impaction/inflammation, not a diagnosis. Differential guided by distribution + chronicity:
- 109. Guidelines Series: GINA Guidelines – Special Considerations in Asthma Care
In this episode, we’re concluding our review of the Global Initiative for Asthma (GINA) guidelines on asthma today with a cased based episode on special considerations in asthma care. We’ve covered asthma diagnosis and phenotyping, the approach to therapy inhaler and oral medical therapy, and biologic therapy. On today’s episode we’re talking about complex cases that are at the edges of the guidelines, or may be in future guidelines. To help us with this exciting topic we’re joined by an expert in the field. Enjoy!
Meet Our Guest
Dr. Meredith McCormack is a Professor of Medicine at Johns Hopkins, where she leads multiple NIH funded endeavors at understanding lung health and disease. She is the Division Director for Pulmonary and Critical Care Medicine, while also directing the Asthma Precision Medicine Center of Excellence, and the BREATHE Center, which focuses on understanding the effects of the environment on lung health and disease through research and community engagement. She is an internationally recognized expert in asthma management and is a dedicated member of the faculty who is committed to the trainees.
Meet Our Co-Hosts
Rupali Sood grew up in Las Vegas, Nevada and made her way over to Baltimore for medical school at Johns Hopkins. She then completed her internal medicine residency training at Massachusetts General Hospital before returning back to Johns Hopkins, where she is currently a second year pulmonary and critical care medicine fellow alongside Tom. Rupali’s interests include interstitial lung disease, particularly as related to oncologic drugs. And she also loves bedside medical education.
Tom Di Vitantonio is originally from New Jersey and attended medical school at Rutgers, New Jersey Medical School in Newark. He then completed his internal medicine residency at Weill Cornell, where he also served as a chief resident. He currently is a second year pulmonary and critical care medicine fellow at Johns Hopkins, and he’s passionate about caring for critically ill patients, how we approach the management of pulmonary embolism, and also about medical education of trainees to help them be more confident and patient centered in the care they have going forward.
Key Learning Points
Episode themes
Built on GINA 2024: final capstone focusing on evolving topics + case-based application.
Three focal areas: (1) obesity/metabolic health (GLP-1s, metformin), (2) dual biologics vs switching, (3) de-escalating inhalers while on biologics.
Emphasis throughout on personalized care, shared decision-making, and multidisciplinary collaboration.Obesity & metabolic health in asthmaObesity affects mechanics, inflammation, and treatment response; tackling metabolic dysfunction can improve asthma control.
GLP-1 receptor agonists may provide additive benefit beyond weight loss for some patients (early clinical signals; trials ongoing).
Metformin is being studied as a potential adjunct targeting metabolic-inflammatory pathways.
Practical approach: screen/counsel on weight, activity, and metabolic disease; partner with primary care/endocrine/sleep clinics; consider GLP-1/other agents when indicated for comorbidities, with potential asthma “bonus.”
Biologics: switching vs dual therapyConsider switching/adding when control is not achieved or sustained on a biologic despite adherence.
Upstream vs downstream targets:- Upstream: anti-TSLP (e.g., tezepelumab) may help when multiple pathways/biomarkers (e.g., high IgE + eos) suggest broader blockade.Downstream: IL-5/IL-4/13/IgE agents selected to match phenotype/endotypes.
Comorbidities can drive choice:- Nasal polyps or upper airway syndromes: there are biologic options that improve upper airway symptoms in addition to asthmaAtopic dermatitis: agents with dual indications can be life-changing.
Logistics matter: injection burden/needle phobia and dosing cadence (e.g., every 2 vs 4–8 weeks) can determine real-world success.De-escalating inhalers on biologicsDon’t step down immediately. Ask patients to maintain their full regimen for ~3 months after starting a biologic to gauge true benefit.Set expectations early and share a step-down plan to prevent unsupervised discontinuation.Typical order (individualize):- Remove non-essential add-ons first (e.g., antihistamines, leukotriene modifiers).Reduce ICS dose gradually (high → medium → low).Keep ICS/LABA combination among the last therapies to taper
Targets while stepping down: “normal” lung function when feasible, minimal/no day or night symptoms, full activity, no exacerbations.
When patients don’t respond to biologicsRe-check the fundamentals:- Adherence/technique for inhalers and biologic.Biomarkers behaving as expected (e.g., eosinophils falling on anti-IL-5).Revisit the diagnosis and contributors/mimics (e.g., vocal cord dysfunction, upper-airway disease).
- Consider moving upstream (e.g., to TSLP) if a downstream agent underperforms.
Communication & practical pearls
- Use visual aids to verify what patients actually take and how (e.g., Asthma & Allergy Network inhaler pictogram).
- Needle issues are common; home vs clinic administration and family support can make or break adherence.
- Biologics are transformative for the right patient—consider them early in steroid-dependent or poorly controlled severe asthma.
- Think longitudinally: plan for monitoring, comorbidity management, and timely adjustments.
28 October 2025, 4:15 am - 18 minutes 37 seconds108. Journal Club with BMJ Thorax – Bronchiectasis
We’re back with our 4th episode in our collaborative series with BMJ Thorax. This week’s episode covers four articles related to bronchiectasis and covers a range of topics in this domain including novel therapeutics, registry data to understand risk, and health related quality of life.
Our mission at Pulm PEEPs is to disseminate and promote pulmonary and critical care education, and we highly value the importance of peer reviewed journals in this endeavor. Each month in BMJ Thorax, a journal club is published looking at high yield and impactful publications in pulmonary medicine. We will be putting out quarterly episodes in association with Thorax to discuss a journal club publication and synthesize four valuable papers.

Meet Our Guests
Chris Turnbull is an Associate Editor for Education at Thorax. He is an Honorary Researcher and Respiratory Medicine Consultant at Oxford University Hospitals. In addition to his role as Associate Editor for Education at BMJ Thorax, he is also a prominent researcher in sleep-related breathing disorders.
Dr. George Doumat completed his medical school at the American University of Beirut and now is an internal medicine resident at UT south western in his second year of training. Prior to starting residency he was a research fellow at MGH studying chronic lung disease.
Journal Club Papers
- Journal club paper from BMJ Thorax
- Phase 3 Trial of the DPP-1 Inhibitor Brensocatib in Bronchiectasis
- Cathepsin C (dipeptidyl peptidase 1) inhibition in adults with bronchiectasis: AIRLEAF, a phase II randomised, double-blind, placebo-controlled, dose-finding study
- Five-Year Outcomes among U.S. Bronchiectasis and NTM Research Registry Patients
- Anxiety, depression, physical disease parameters and health-related quality of life in the BronchUK national bronchiectasis cohort
To submit a journal club article of your own to Thorax, you can contact Chris directly – [email protected]
To engage with Thorax, please use the social media channels (Twitter – @ThoraxBMJ; Facebook – Thorax.BMJ) and subscribe on your preferred platform, to get the latest episodes directly on your device each month.Key Learning Points
- Four recent papers (2 RCTs, 2 large cohorts) chosen to show both new therapeutics and real-world comorbidities/outcomes, pushing toward precision medicine.
1) ASPEN trial – brensocatib (DPP-1 inhibitor)
- Design: Phase 3, ~1,700 pts, 35 countries, 52 weeks; stratified randomization by region.
- Results: ↓ annualized exacerbation rate (~1.0 vs 1.3/yr; RR≈0.8), longer time to first exacerbation, ~10% absolute ↑ in “exacerbation-free” patients at 1 year, QoL improved, modest FEV1 decline difference (~40 mL/yr).
- Take: First targeted therapy with consistent benefit; effect on lung function small but directionally supportive.
- Gaps: Need long-term durability, adolescent data, and comparisons/positioning in pts with asthma/COPD overlap.
2) AIRLEAF (BI 1291583) – reversible cathepsin C inhibitor
- Design: Phase 2, 4 arms (3 doses + placebo), model-based dose–response analysis to optimize dose selection.
- Results: Overall dose–response signal; individual low-dose arms trended to fewer exacerbations but not statistically significant; skin events more common at higher doses.
- Take: Promising class targeting neutrophil pathway, but needs Phase 3 before clinical use.
3) U.S. Bronchiectasis & NTM Registry – 5-year outcomes
- Cohort: >2,600 CT-confirmed; ~59% with baseline NTM identified.
- Results: 5-yr mortality ~12%; no mortality difference with vs without NTM; predictors = lower baseline FEV1, older age, male sex, prior hospitalization. FEV1 decline ~38 mL/yr. Baseline NTM group had fewer exacerbations (counterintuitive).
- Interpretation cautions: Likely mix of colonization vs active disease; referral/management effects in specialized centers; registry strengths (size, real-world, longitudinal) vs pitfalls (confounding, data quality, causality).
4) Bronch-UK cohort – anxiety & depression
- Cohort: 1,340 adults; HADS screening.
- Prevalence: Anxiety ~33%, depression ~20%; many undiagnosed (≈26%/16%).
- Impact: Worse QoL, more severe disease; depression ~1.8× higher hospitalization risk and shorter time to severe exacerbation.
- Caveat: Association ≠ causation; sicker patients may have more mental health burden.
Practical takeaways for clinic
- Consider brensocatib for appropriate non-CF bronchiectasis patients once accessible; frame benefits around fewer exacerbations and QoL, not big lung function gains.
- Do not introduce cathepsin C inhibitors outside trials yet; discuss as pipeline only.
- Risk stratify using FEV1, age, sex, and prior hospitalizations; expect ~40 mL/yr average FEV1 decline.
- Screen mental health routinely (HADS, PHQ-9, GAD-7). Build multidisciplinary pathways; consider brief CBT-style supports embedded in bronchiectasis clinics, with targeted referrals.
- Registry data ≠ RCTs: Use for counseling and service design, but avoid causal claims.
Research/implementation gaps highlighted
- Long-term safety/efficacy and subgroup effects for brensocatib (adolescents, asthma/COPD overlap).
- Phase 3 confirmation for cathepsin C inhibition and dose selection.
- Granular NTM phenotyping (colonization vs disease) to reconcile paradoxical exacerbation signals.
- Scalable mental-health interventions integrated into respiratory clinics; trials to test impact on exacerbations/hospitalizations.
Pro tip from the episode
When appraising trials, check the CONSORT diagram for generalizability and look for stratification methods in multinational RCTs; in phase 2 programs, expect model-based dose–response designs that trade breadth for power.
7 October 2025, 4:30 am - 107. Fellows’ Case Files: University of Kansas Medical Center KUMC
After a brief hiatus, we are excited to be back today with another Fellows’ Case Files! Today we’re virtually visiting the University of Kansas Medical Center (KUMC) to hear about a fascinating pulmonary presentation. There are some fantastic case images and key learning points. Take a listen and see if you can make the diagnosis along with us. As always, let us know your thoughts and definitely reach out if you have an interesting case you’d like to share.
Meet Our Guests
Dr. Vishwajit Hegde completed his internal medicine residency at University of Kansas Medical Center where he stayed for fellowship and is currently a second year Pulmonary and Critical Care medicine fellow.
Dr. Sahil Pandya is an Associate Professor of Medicine and Program Director of the PCCM Fellowship at KUMC.
Case Presentation
Imaging



Infographic
Key Learning Points
1) Initial frame & diagnostic mindset
- Young (26), subacute → chronic dyspnea/cough with diffuse pulmonary nodules; avoid premature closure on TB.
- Use a Bayesian approach: combine pre-test probability (epidemiology, exposures, tempo) with targeted tests to decide next steps.
- Always confirm TB when possible (micro/path + resistance testing); empiric RIPE may be reasonable but shouldn’t replace tissue when stakes are high.
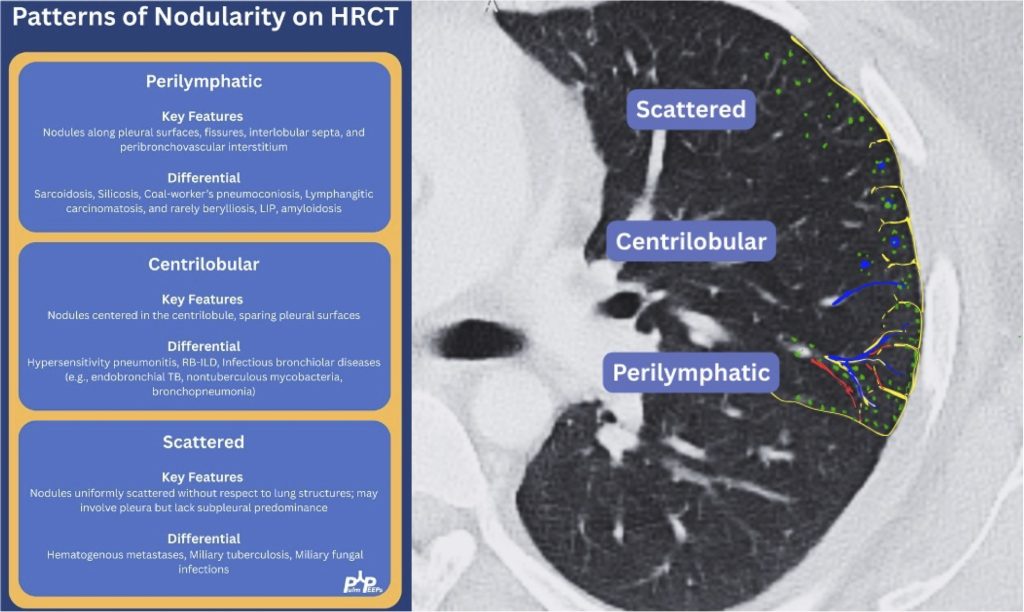
2) Imaging pearls—nodular pattern recognition
- Ask three things: craniocaudal distribution, symmetry, central vs peripheral.
- Centrilobular (spares pleura/fissures): airway-centered (e.g., NTM, bronchiolitis, tree-in-bud).
- Perilymphatic (tracks fissures/pleura & septa): sarcoid, lymphangitic spread.
- Random/diffuse (involves pleural surfaces): hematogenous spread → think miliary TB, disseminated fungal, septic emboli, metastatic disease.
- Interval change matters: new cavitation and confluence can upweight infection or aggressive malignancy.
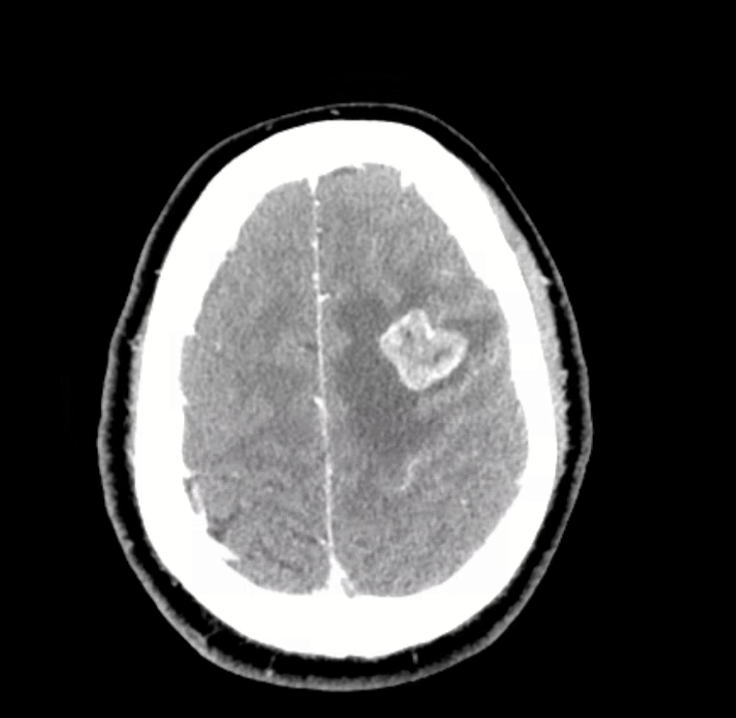
3) Neuro findings—ring-enhancing lesions
- Differential: septic emboli/abscess, nocardia, fungal, TB, parasites, metastases, vasculitis, sarcoid.
- Partner with neuroradiology for pattern nuances; treat seizures but keep searching for the unifying diagnosis.
4) Lab/serology strategy
- Broad infectious workup (AFB × multiple, fungal serologies), HIV and basic immune screen.
- Negative/indeterminate tests don’t end the search—revisit history (e.g., Ohio travel → histo/blasto risk).
5) “Tissue is the issue”—choosing the procedure
- For diffuse nodules with mediastinal adenopathy and stable patient: EBUS-TBNA + BAL, consider transbronchial or cryobiopsy.
- Cryobiopsy pros: larger, less crush artifact, better for molecular testing; cons: ↑ bleeding/pneumothorax vs forceps.
- VATS still best for certain ILD questions or if less invasive routes are non-diagnostic—but weigh patient preference and stage/likelihood of yield.
6) ROSE (rapid on-site evaluation) in bronchoscopy
- Confirms adequacy in real time, steers you away from necrotic zones, helps decide when you’ve got enough for molecular studies, and when to pivot sites—reduces anesthesia time and repeat procedures.
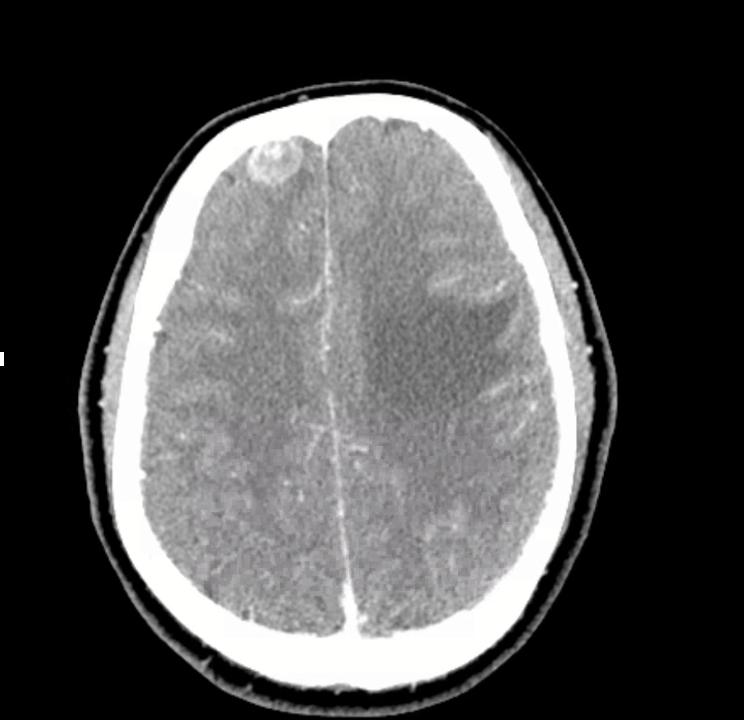
7) Final diagnosis & management
- Path: TTF-1+, CK7+, napsin A → pulmonary adenocarcinoma with a fusion driver.
- Therapy: Targeted TKI (crizotinib) → dramatic radiographic response of miliary lung disease and CNS lesions.
- Teaching point: even “miliary TB-like” lungs + CNS lesions in a 20-something can be driver-positive lung cancer—don’t let age or pattern blind you.
References and Further Reading
- Desai, S., Devaraj, A., Lynch, D., & Sverzellati, N. (2020). Webb, Müller and Naidich’s high-resolution CT of the lung (6th ed.). Lippincott Williams & Wilkins.
- Rajeswaran, G., Becker, J. L., Michailidis, C., Pozniak, A. L., & Padley, S. P. G. (2006). The radiology of IRIS (immune reconstitution inflammatory syndrome) in patients with mycobacterial tuberculosis and HIV co-infection: appearances in 11 patients. Clinical radiology, 61(10), 833-843
- Poletti, V., Ravaglia, C., & Tomassetti, S. (2016). Transbronchial cryobiopsy in diffuse parenchymal lung diseases. Current opinion in pulmonary medicine, 22(3), 289-296.
- Norman, G. R., Monteiro, S. D., Sherbino, J., Ilgen, J. S., Schmidt, H. G., & Mamede, S. (2017). The causes of errors in clinical reasoning: cognitive biases, knowledge deficits, and dual process thinking. Academic Medicine, 92(1), 23-30.
1 October 2025, 4:15 am - 7 minutes 11 seconds106. Pulm PEEPs Pearls: ICI Pneumonitis
We are so excited to be launching a new series here at Pulm PEEPs! We’ll be talking about high yield topics in 15 minutes or less. In this series, Furf and Monty will tackle core points and provide an overview, key points, and further reading. We’re starting with a key point review of Immune Checkpoint Inhibitor Pneumonitis. Let us know if there are other topics you want to hear about!
Key Learning Points
- Epidemiology & Pathophysiology
-
- Increasingly common as immunotherapy use grows in oncology.
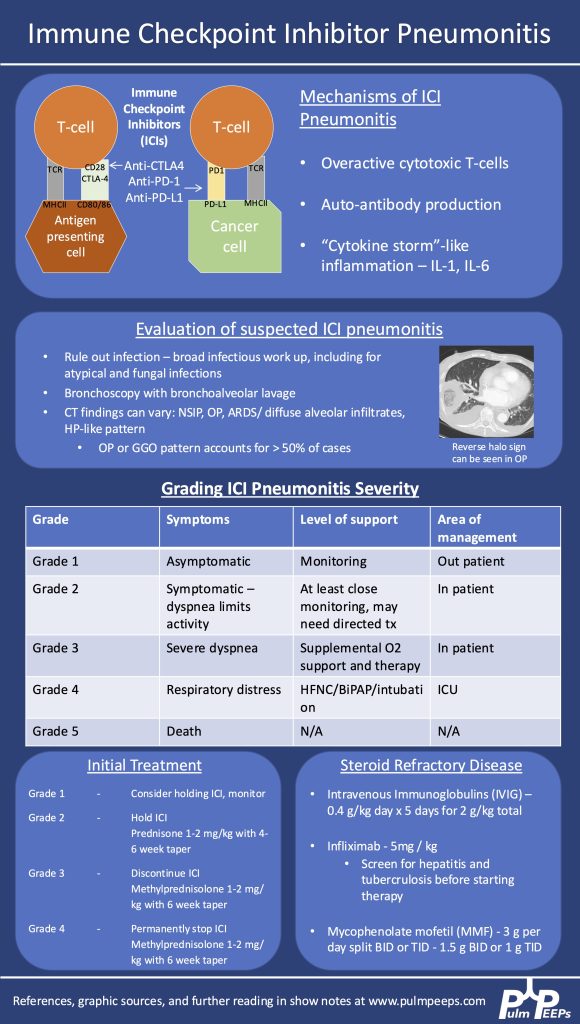
- Caused by immune activation from PD-1, PD-L1, or CTLA-4 inhibitors.
- Mechanisms:
- Overactive T cells
- Autoantibody production
- Cytokine-mediated inflammation (e.g., ↑IL-1, ↑IL-6)
- Clinical Suspicion & Diagnosis
-
- Any new respiratory symptoms in a patient currently or previously on ICI → consider ICI pneumonitis.
- CT findings are variable: can mimic organizing pneumonia, NSIP, ARDS, or diffuse ground glass opacities. Imaging pattern does not determine severity grade.
- Diagnosis is of exclusion — infection and malignancy progression must be ruled out first.
- Workup:
- Broad infectious evaluation (cultures, viral panel, fungal markers).
- Early bronchoscopy with BAL if feasible — typically lymphocyte-predominant in ICI pneumonitis.
- Screen for TB and hepatitis early (in case infliximab is needed).
- Severity Grading (Symptom- & O₂-based, not imaging-based)
-
- Grade 1: Asymptomatic → monitor, may hold ICI.
- Grade 2: Symptomatic but not hypoxic → prednisone 1 mg/kg/day PO.
- Grade 3–4: Hypoxemia or ICU-level care → methylprednisolone 1–2 mg/kg/day IV. Usually hold or permanently stop ICI.
- Steroid Management
-
- Typical taper: over 6 weeks for grade ≥3.
- Week 1: 1–2 mg/kg/day
- Gradual step-down to 0.25 mg/kg/day by week 5, then stop week 6.
- Chronic/recurrent cases may need slower tapers over months.
- Add GI prophylaxis and PJP prophylaxis during prolonged steroid use.
- Typical taper: over 6 weeks for grade ≥3.
- If Steroids Fail (no improvement after 48–72 hrs)
-
- Consider adding:
- IVIG (2 g/kg over 5 days)
- Infliximab (TNF-α inhibitor — requires TB/hepatitis screening)
- Mycophenolate mofetil (1–1.5 g/day BID or TID, start at effective dose quickly)
- IVIG may have lower mortality in some series but comes with risks (volume overload, thrombosis, infusion reactions).
- Consider adding:
- Emerging Therapies
-
- JAK inhibitors are under investigation as possible future options.
- Multidisciplinary Care
-
- ICU management is a team sport — coordinate with oncology, critical care, infectious disease, and pharmacy.
Infographic
References and Further Reading
- Managing Immune Checkpoint Inhibitor Pneumonitis in the ICU. Montemayor, Kristina et al.CHEST Critical Care, Volume 3, Issue 1, 100126
- Lavalle S, Masiello E, Valerio MR, Aliprandi A, Scandurra G, Gebbia V, Sambataro D. Immune checkpoint inhibitor therapy‑related pneumonitis: How, when and why to diagnose and manage (Review). Exp Ther Med. 2024 Jul 30;28(4):381. doi: 10.3892/etm.2024.12670. PMID: 39113908; PMCID: PMC11304171.
- Delaunay M, Prévot G, Collot S, Guilleminault L, Didier A, Mazières J. Management of pulmonary toxicity associated with immune checkpoint inhibitors. Eur Respir Rev. 2019 Nov 6;28(154):190012. doi: 10.1183/16000617.0012-2019. PMID: 31694838; PMCID: PMC9488507.
12 August 2025, 4:30 am - 23 minutes 53 seconds105. ICU Acquired Weakness
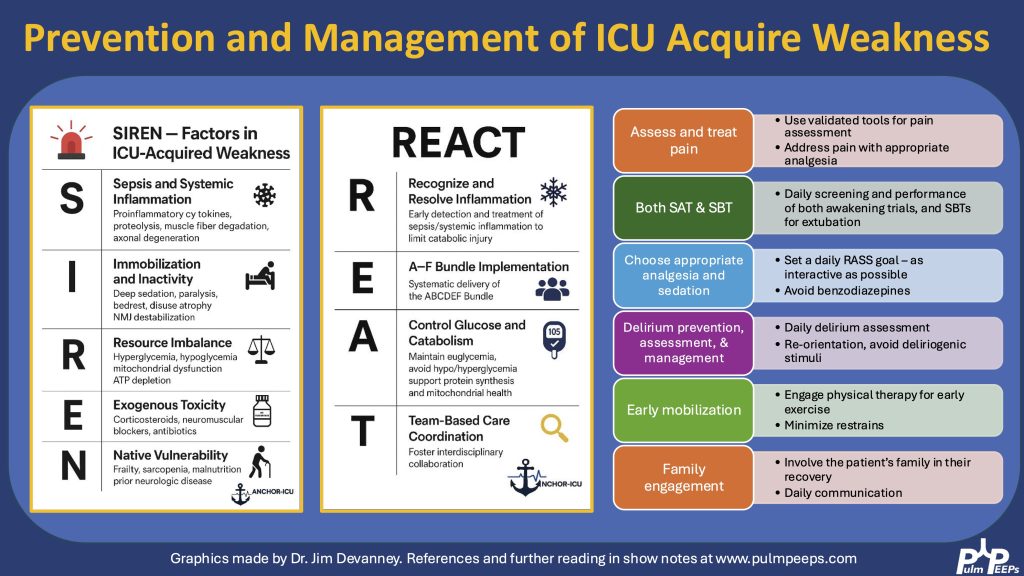
Today we’re talking about a topic that is relevant for all critical care physicians but under-examined: ICU Acquired Weakness. We are joined by two excellent guests to walk through a case and discuss the diagnosis, pathophysiology, prevention, and treatment of ICU Acquired Weakness. Check out our associated infographics and key learning points below.
Meet Our Guests
Jim Devanney is a Physiatrist who just completed a neurocritical care fellowship at BIDMC. He is transitioning to a clinical associate position at University Health Network – University of Toronto where he will be working as a PM&R consultant within the ICU.
Kalaila Pais is a third year internal medicine resident at BIDMC, interested in pulmonary and critical care and medical education and is returning for her third Pulm PEEPs episode.
Key Learning Points
Definition & Clinical Presentation
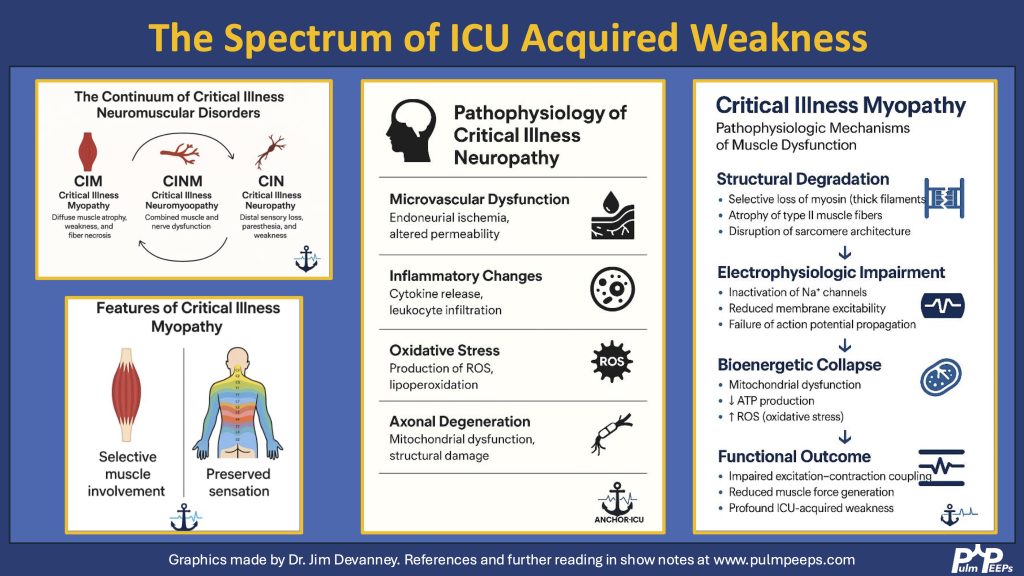
ICU-AW refers to new-onset, generalized muscle weakness that arises during critical illness, not explained by other causes.It typically presents as:- Symmetric, proximal > distal weaknessRespiratory muscle involvementPreserved cranial nerve functionNo sensory deficits in myopathy (sensory loss points toward neuropathy)
- Muscle dysfunctionEarly onset (within 48 hrs)Sensation intactproximal > distal weakness
Critical Illness Polyneuropathy (CIP):- Nerve involvementDistal > proximal weakness, sensory deficits
- Critical Illness Polyneuromyopathy (CIPNM): Combination of both
Diagnosis
- Medical Research Council Score (MRC-SS):
- Score < 48: ICU-AW
- Score < 36: severe ICU-AW
- Handgrip dynamometry: <11 kg (men), <7 kg (women)
- Electrophysiology: EMG/NCS to distinguish CIM vs CIP
- Muscle ultrasound: bedside monitoring
- MRI/CT/Muscle biopsy: rarely used due to practical limitation
Risk Factors
Modifiable:
- Hyper/hypoglycemia
- Electrolyte derangement
- Parenteral nutrition
- Immobility
- Medications (steroids, NM blockers, sedatives, aminoglycosides)
Non-modifiable:
- Age, female sex, comorbidities
- Severity of illness, prolonged ventilation
- Sepsis, multi-organ failure
Management & Prevention
- Prevention is key:
- Early treatment of sepsis and inflammation
- Glycemic control
- Early enteral nutrition
- Minimize sedation (A-F bundle)
- Early mobilization and physical therapy
- NMES (neuromuscular electrical stimulation): emerging therapy, needs more evidence
Outcomes
- Short-term: increased LOS, ventilation duration, mortality
- Long-term: decreased function, discharge to rehab, prolonged recovery
Final Takeaways
- Prevention is crucial — start interventions early.
- Systematic approach to ICU weakness helps rule out dangerous mimics.
- ICU-AW is common but often under-recognized — awareness and early rehab can significantly impact recovery.
Infographics
References and Further Reading
Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Devlin JW, Skrobik Y, Gélinas C, et al. Critical Care Medicine. 2018;46(9):e825-e873. doi:10.1097/CCM.0000000000003299.The ABCDEF Bundle: Science and Philosophy of How ICU Liberation Serves Patients and Families. Ely EW. Critical Care Medicine. 2017;45(2):321-330. doi:10.1097/CCM.0000000000002175.
Caring for Critically Ill Patients With the ABCDEF Bundle: Results of the ICU Liberation Collaborative in Over 15,000 Adults. Pun BT, Balas MC, Barnes-Daly MA, et al. Critical Care Medicine. 2019;47(1):3-14. doi:10.1097/CCM.0000000000003482.
Delirium in Critical Illness: Clinical Manifestations, Outcomes, and Management. Stollings JL, Kotfis K, Chanques G, et al. Intensive Care Medicine. 2021;47(10):1089-1103. doi:10.1007/s00134-021-06503-1.
ICU-acquired Weakness. Vanhorebeek I, Latronico N, Van den Berghe G. Intensive Care Medicine. 2020;46(4):637-653. doi:10.1007/s00134-020-05944-4.
Clinical Review: Intensive Care Unit Acquired Weakness. Hermans G, Van den Berghe G. Critical Care (London, England). 2015;19:274. doi:10.1186/s13054-015-0993-7.
Best Practices for Conducting Interprofessional Team Rounds to Facilitate Performance of the ICU Liberation (ABCDEF) Bundle. Stollings JL, Devlin JW, Lin JC, et al. Critical Care Medicine. 2020;48(4):562-570. doi:10.1097/CCM.0000000000004197.
ABCDE and ABCDEF Care Bundles: A Systematic Review of the Implementation Process in Intensive Care Units. Moraes FDS, Marengo LL, Moura MDG, et al. Medicine. 2022;101(25):e29499. doi:10.1097/MD.0000000000029499.
29 July 2025, 4:30 am - 18 minutes 38 seconds104. Pulm PEEPs on Core IM – Pleural Effusions
Hi Pulm PEEPs! Today we have a special episode for you. Monty and Furf were invited on the Core IM Podcast to talk about the work up and management of pleural effusions. This is a great overview and we hope you enjoy listening as much as we did recording. If you want a deeper dive into pleural effusions check out our prior series:
36. Top Consults Series: Approach to Pleural Effusions
37. Top Consults: Approach to Parapneumonic Effusions
49. Top Consults: Malignant Pleural Effusions
 9 July 2025, 4:30 am
9 July 2025, 4:30 am - 26 minutes 58 seconds103. Fellows’ Case Files: University of Virginia
Today, we’re virtually visiting the University of Virginia for another Fellows’ Case Files. This is a fantastic case that covers ARDS, the infectious work up of an immunosuppressed patient, and the evaluation of undifferentiated shock. Please let us know what you think of the episode and always feel free to reach out with interesting cases!
Meet Our Guests
John Popovich completed his residency training and chief year at UVA and has stayed on there for his pulmonary and critical care fellowship.
Tim Scialla is an associate professor of medicine at UVA. He completed his residency and fellowship at Johns Hopkins Hospital where he was also an ACS. His clinical and research focuses are advanced airways disease. He is also the program director of the PCCM fellowship.
Matt Freedman completed his residency training at Virginia Commonwealth University and is currently a second year fellow at University of Virginia.
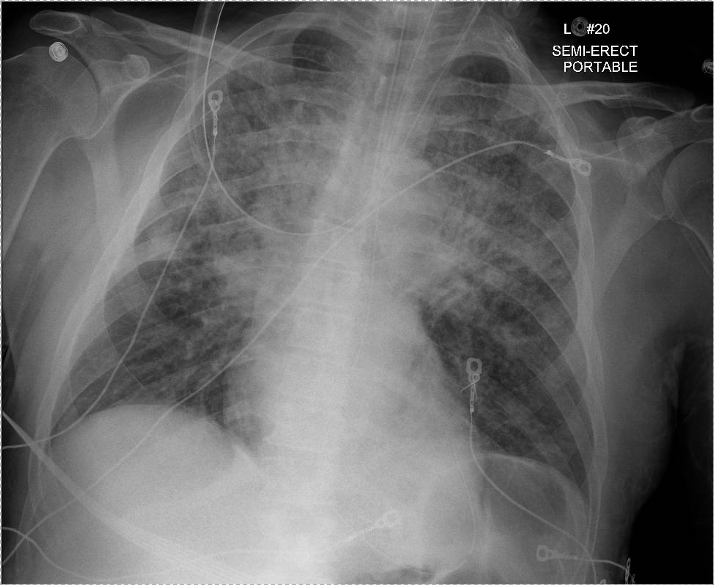
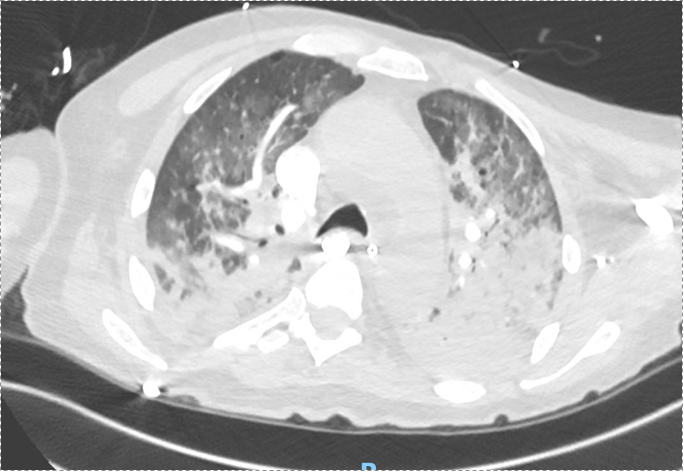
Case Presentation
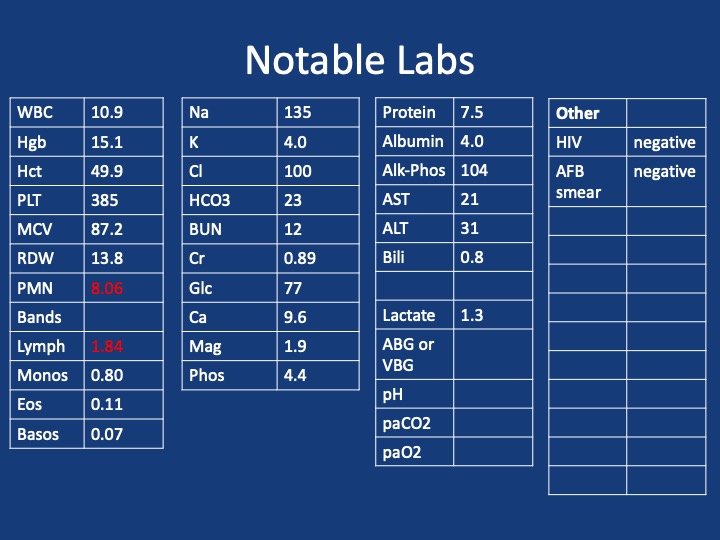
Patient: 52-year-old male with psoriasis, HIV/AIDS (CD4 count: 71), presenting with progressive shortness of breath, fever, non-productive cough, and weight loss.
Vital signs: Febrile (103°F), tachycardic (HR 110), hypoxemic on 6L O₂ (SpO₂ 90–92%).
Exam: Diffuse crackles, ill-appearing.
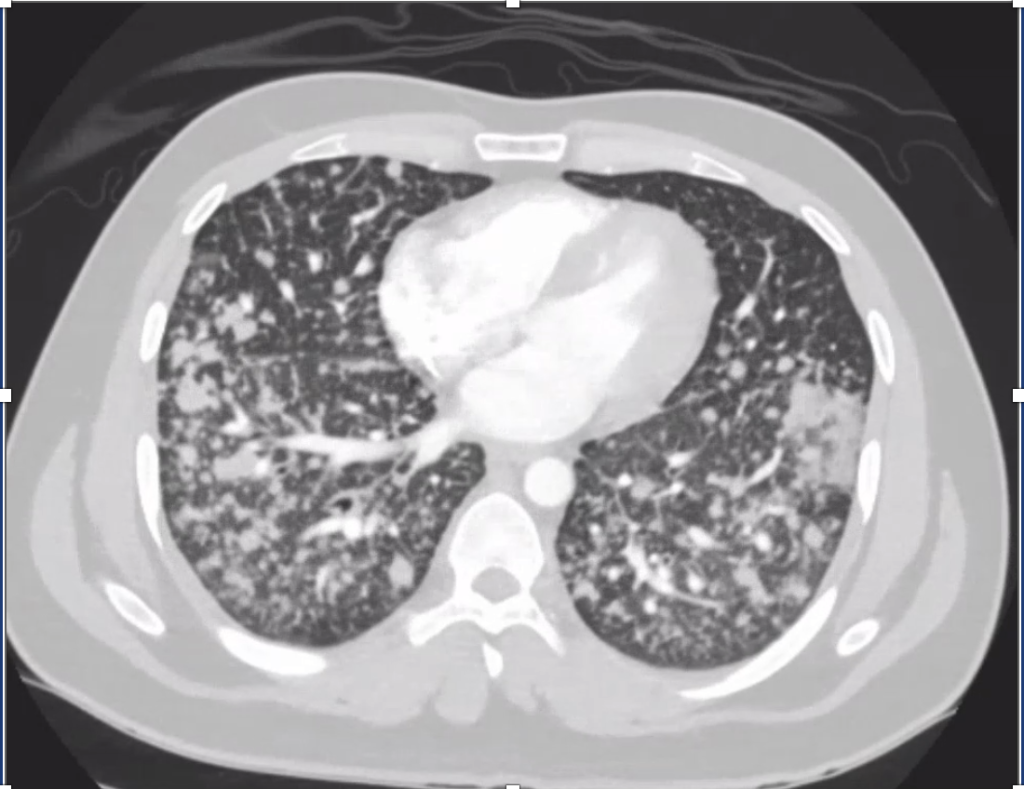
Imaging: CXR and CT showed bilateral upper lobe infiltrates, ground-glass opacities, septal thickening, and peripheral cystic changes.

Infographics
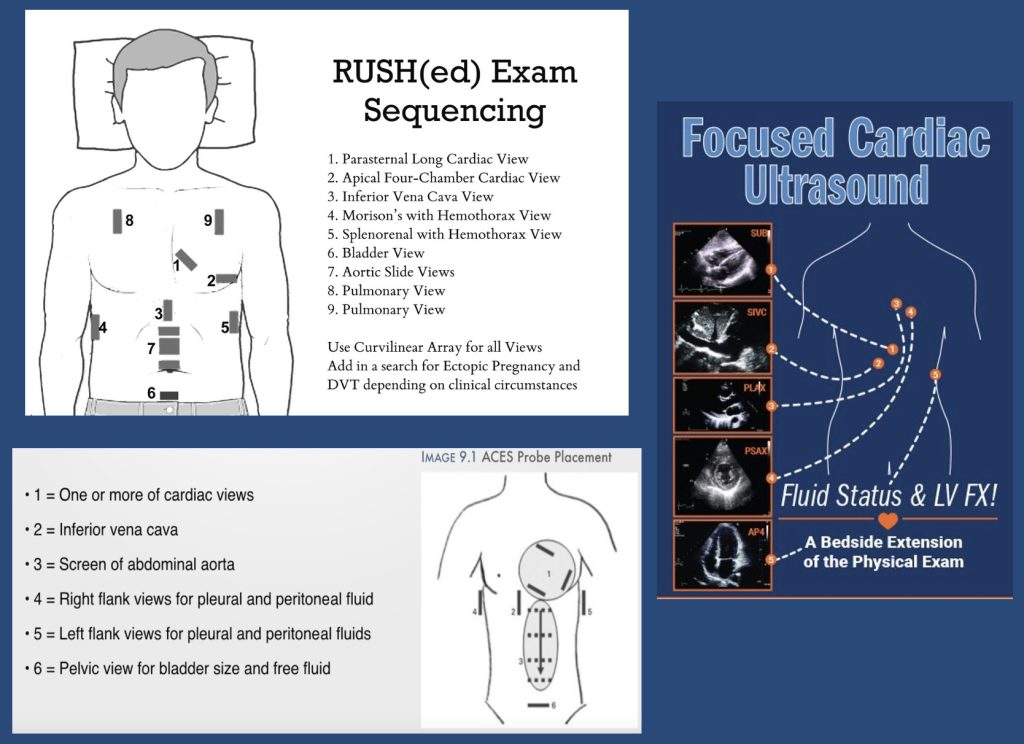 POCUS algorithms for investigating shock
POCUS algorithms for investigating shock
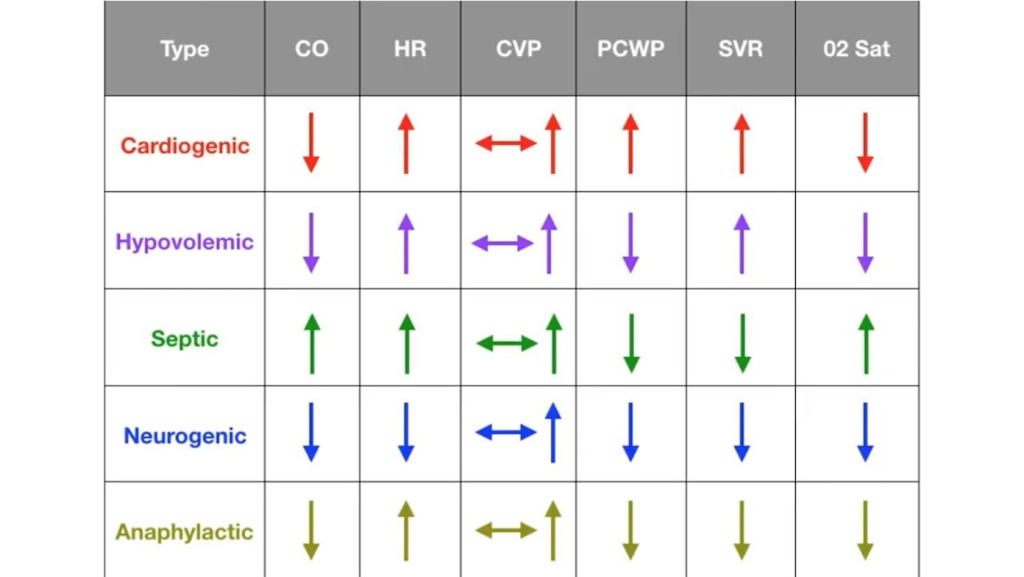
Shock physiology:
Key Learning Points
Diagnostic Reasoning in Immunocompromised Hosts
- Framework: Anchor the differential based on type of immunosuppression.
- HIV/AIDS → T-cell dysfunction, affecting susceptibility to PCP, TB, CMV, fungi (e.g. histo/blasto), and common CAP organisms.
- PCP considerations:
- PCP can occur despite prophylaxis (e.g. Bactrim), especially if adherence or resistance issues exist.
- Classic symptoms in AIDS: acute, febrile, hypoxemic respiratory failure.
Use of Serum Markers and Imaging
- LDH: Elevated in PCP, but non-specific. High negative predictive value when normal.
- 1,3-β-D-glucan: Elevated in PCP and other fungal infections. Very sensitive for PCP (up to 95%).
- Imaging: Ground-glass opacities with cystic changes support PCP diagnosis.
Role of Bronchoscopy and Diagnostic Yield
- BAL studies to obtain:
- DFA for PCP (rapid, high specificity, lower sensitivity)
- PCR for PCP (higher sensitivity, slower turnaround)
- Cultures: bacterial, fungal, mycobacterial
- Cytology, galactomannan, histo/blasto urine antigens
- Bronch Risk-Benefit:
- Can change management in 40–60% of cases.
- Complication rate: ~10–15%, most often hypoxemia.
- Heuristic for pre-bronch ABG on non-rebreather:
- PaO₂ >150 → likely safe
- 100–150 → ~25% risk of intubation
- <100 → high risk of decompensation
Steroids in PCP and Severe CAP
- Steroids indicated in PCP with significant hypoxemia (PaO₂ <70 mmHg).
- With new CAP guidelines (Cape Cod trial), steroids may also be considered in severe bacterial CAP.
Shock Evaluation in ICU
- Framework: Simplify into likely causes — distributive most common, but rule out cardiogenic, obstructive, hypovolemic.
- Physical exam + POCUS essential early.
- POCUS: cardiac views, IVC, lung US, abdominal free fluid.
- Low EF doesn’t exclude distributive shock.
- PA catheter (Swan) utility:
- Useful when physiology unclear or when tracking response to therapy is critical.
- Swan data in this patient: low CVP and wedge, high SVR → distributive shock, not cardiogenic despite low EF.
1 July 2025, 4:30 am - Framework: Anchor the differential based on type of immunosuppression.
- 22 minutes 8 seconds102. Journal Club with BMJ Thorax – Sleep and Non-Invasive Ventilation
Today is our third episode in our collaborative series with BMJ Thorax. Our mission at Pulm PEEPs is to disseminate and promote pulmonary and critical care education, and we highly value the importance of peer reviewed journals in this endeavor. Each month in BMJ Thorax, a journal club is published looking at high yield and impactful publications in pulmonary medicine. We will be putting out quarterly episodes in association with Thorax to discuss a journal club publication and synthesize four valuable papers. This week’s episode covers four articles related to obstructive sleep apnea therapies, and the use of non-invasive ventilation and high flow nasal cannula for intubation and COPD exacerbations.

Meet Our Guests
Chris Turnbull is an Associate Editor for Education at Thorax. He is an Honorary Researcher and Respiratory Medicine Consultant at Oxford University Hospitals. In addition to his role as Associate Editor for Education at BMJ Thorax, he is also a prominent researcher in sleep-related breathing disorders.
Natalie McLeod is a resident in respiratory medicine and is currently doing a clinical fellowship in sleep and ventilation at Oxford University Hospitals.
Journal Club Papers
- Journal club article from Thorax
- Effect of CPAP therapy on blood pressure in patients with obstructive sleep apnoea: a worldwide individual patient data meta-analysis
- Hypoglossal nerve stimulation for obstructive sleep apnea in adults: An updated systematic review and meta-analysis
- Noninvasive Ventilation for Preoxygenation during Emergency Intubation
- Nasal high flow or noninvasive ventilation? navigating hypercapnic COPD exacerbation treatment: A randomized noninferiority clinical trial
To submit a journal club article of your own to Thorax, you can contact Chris directly – [email protected]
To engage with Thorax, please use the social media channels (Twitter – @ThoraxBMJ; Facebook – Thorax.BMJ) and subscribe on your preferred platform, to get the latest episodes directly on your device each month.17 June 2025, 4:30 am - More Episodes? Get the App