🚀 From Google Podcasts to Moon FM in No Time: Your Hassle-Free Migration Guide
👉

Cardionerds is a medical cardiology podcast and platform that democratizes cardiovascular education and brings high yield cardiovascular concepts in a fun and engaging format to listeners of all levels.
CardioNerds (Drs. Gurleen Kaur and Richard Ferraro) and episode FIT Lead Dr. Spencer Carter (Cardiology Fellow at UT Southwestern) discuss the clinical implementation of GLP-1 receptor agonists with Dr. Neha Pagidapati (Faculty at Duke University School of Medicine). In this episode of the CardioNerds Cardiovascular Prevention Series, we discuss the clinical implementation of glucagon-like peptide-1 (GLP-1) receptor agonists. We cover the clinical indications, metabolic and cardiovascular benefits, and potential limitations of these emerging and exciting therapies. Show notes were drafted by Dr. Spencer Carter. Audio editing was performed by CardioNerds Academy Intern, student Dr. Pacey Wetstein.
This episode was produced in collaboration with the American Society of Preventive Cardiology (ASPC) with independent medical education grant support from Novo Nordisk. See below for continuing medical education credit.
Claim CME for this episode HERE.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Prevention Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
What were the groundbreaking findings of the STEP1 and SURMOUNT-1 trials and how these impact cardiovascular wellness?
What were the findings of the LEADER trial and their implications for patients with type II diabetes and high cardiovascular risk?
What are current indications for GLP1 agonists in the context of cardiometabolic disease.
What are important side effects or contraindications to GLP1 agents when used for cardiovascular risk reduction and wellness?
What are practical concerns associated with GLP-1 use, and how can these be overcome?
CardioNerds (Dr. Dan Ambinder), Dr. Nino Isakadze (EP Fellow at Johns Hopkins Hospital), and Dr. Karan Desai (Cardiology Faculty at Johns Hopkins Hospital) join Digital Health Experts, Dr. Alexis Beatty (Cardiologist and associate professor in the department of epidemiology and biostatistics at UCSF) and Dr. Seth Martin (Director of the Johns Hopkins Center for Mobile Technologies to Achieve Equity in Cardiovascular Health (mTECH), which is part of the American Heart Association (AHA) Strategically Focused Research Networks on Health Technology & Innovation) for another installment of the Digital Health Series. In this specific episode, we discuss pearls, pitfalls, and everything in between for emerging digital health innovators. This series is supported by an ACC Chapter Grant in collaboration with Corrie Health. Audio editing by CardioNerds Academy Intern, student doctor Shivani Reddy.
In this series, supported by an ACC Chapter Grant and in collaboration with Corrie Health, we hope to provide all CardioNerds out there a primer on the role of digital heath in cardiovascular medicine. Use of versatile hardware and software devices is skyrocketing in everyday life. This provides unique platforms to support healthcare management outside the walls of the hospital for patients with or at risk for cardiovascular disease. In addition, evolution of artificial intelligence, machine learning, and telemedicine is augmenting clinical decision making at a new level fueling a revolution in cardiovascular disease care delivery. Digital health has the potential to bridge the gap in healthcare access, lower costs of healthcare and promote equitable delivery of evidence-based care to patients.
This CardioNerds Digital Health series is made possible by contributions of stellar fellow leads and expert faculty from several programs, led by series co-chairs, Dr. Nino Isakadze and Dr. Karan Desai.

CardioNerds Digital Health Series Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
Immunotherapy is a type of novel cancer therapy that leverages the body’s own immune system to target cancer cells. In this episode, we focused on the most common type of immunotherapy: immune checkpoint inhibitors or ICIs. ICIs are monoclonal antibodies targeting immune “checkpoints” or brakes to enhance T-cell recognition against tumors. ICI has become a pillar in cancer care, with over 100 approvals and 5,000 ongoing trials. ICIs can lead to non-specific activation of the immune system, causing off-target adverse events such as cardiotoxicities. ICI-related myocarditis, though less common, can be fatal in 30% of cases. Clinical manifestations vary but can include chest pain, dyspnea, palpitations, heart failure symptoms, and arrhythmias. Diagnosis involves echocardiography, cardiac MRI, and endomyocardial biopsy. Treatment includes high-dose corticosteroids with potential additional immunosuppressants. Baseline EKG and troponin are recommended before ICI initiation, but routine surveillance is not advised. Subclinical myocarditis is a challenge, with unclear management implications. So let’s dive in and learn about cardiotoxicity of novel immunotherapies with Drs. Giselle Suero (series co-chair), Evelyn Song (episode FIT lead), Daniel Ambinder (CardioNerds co-founder), and Tomas Neilan (faculty expert). Audio editing by CardioNerds Academy Intern, Dr. Maryam Barkhordarian.
This episode is supported by a grant from Pfizer Inc.
This CardioNerds Cardio-Oncology series is a multi-institutional collaboration made possible by contributions of stellar fellow leads and expert faculty from several programs, led by series co-chairs, Dr. Giselle Suero Abreu, Dr. Dinu Balanescu, and Dr. Teodora Donisan.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Cardio-Oncology Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
What are immune checkpoint inhibitors (ICIs)?
What are the cardiotoxicities related to ICI therapies?
What is the general approach to the diagnosis of ICI-myocarditis?
How do endomyocardial biopsy findings for ICI-myocarditis compare to other types of autoimmune-mediated conditions such as transplant rejection?
What are the treatment strategies for ICI-myocarditis?
Can patients be re-treated after an episode of ICI myocarditis?
International Cardio-Oncology Society ( IC-OS). IC-OS exits to advance cardiovascular care of cancer patients and survivors by promoting collaboration among researchers, educators and clinicians around the world. Learn more at https://ic-os.org/.

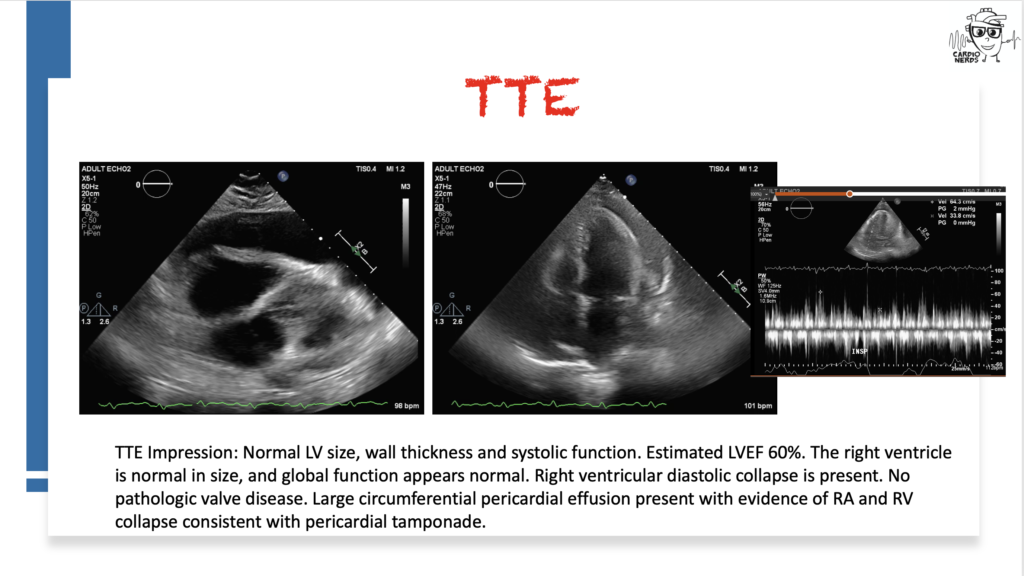
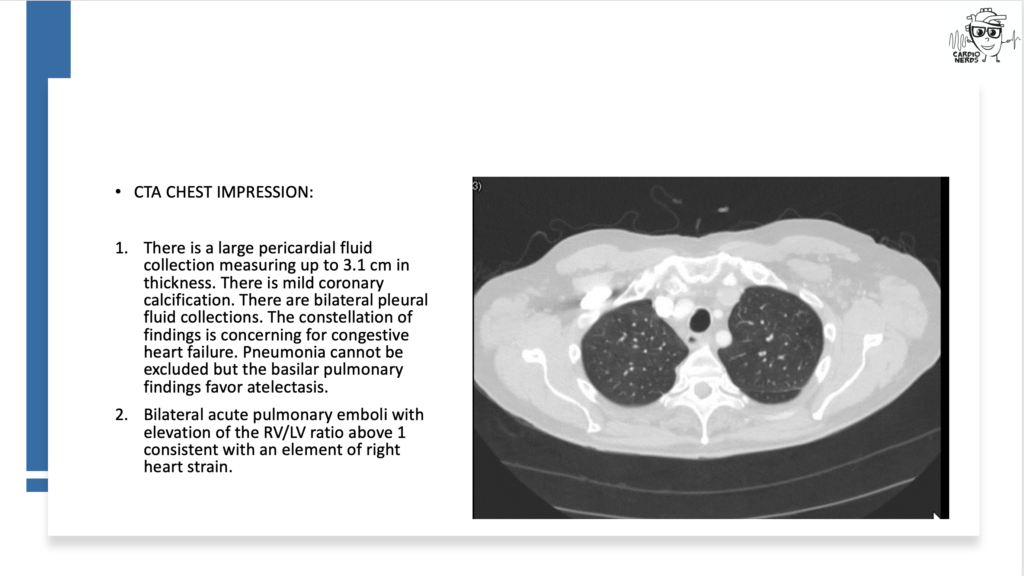
CardioNerds join Dr. Inbar Raber and Dr. Susan Mcilvaine from the Beth Israel Deaconess Medical Center for a Fenway game. They discuss the following case: A 72-year-old man presents with two weeks of progressive dyspnea, orthopnea, nausea, vomiting, diarrhea, and right upper quadrant pain. He has a history of essential thrombocytosis, Barrett’s esophagus, basal cell skin cancer, and hypertension treated with hydralazine. He is found to have bilateral pleural effusions and a pericardial effusion. He undergoes a work-up, including pericardial cytology, which is negative, and blood tests reveal a positive ANA and positive anti-histone antibody. He is diagnosed with drug-induced lupus due to hydralazine and starts treatment with intravenous steroids, resulting in an improvement in his symptoms. Expert commentary is provided by UT Southwestern internal medicine residency program director Dr. Salahuddin (“Dino”) Kazi.
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” – Sir William Osler. CardioNerds thank the patients and their loved ones whose stories teach us the Art of Medicine and support our Mission to Democratize Cardiovascular Medicine.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Case Reports Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
Welcome back to the CardioNerds Cardiovascular Prevention Series, where we are continuing our discussion of Glucagon-like Peptide-1 Receptor Agonists (GLP-1 RAs). This class of medications is becoming a household name, not only for their implications for weight loss but also for their effect on cardiovascular disease. CardioNerds Dr. Ty Sweeney (CardioNerds Academy Faculty Member and incoming Cardiology Fellow at Boston Medical Center), Dr. Rick Ferraro (CardioNerds Academy House Faculty and Cardiology Fellow at Johns Hopkins Hospital), and special guest Dr. Franck Azobou (Cardiology Fellow at UT Southwestern) sat down with Dr. Darren McGuire (Cardiologist at UT Southwestern and Senior Editor of Diabetes and Vascular Disease Research) to discuss important trial data on GLP-1 RAs in patients with heart disease, as well as recent professional society guidelines on their use. Show notes were drafted by Dr. Ty Sweeney. Audio editing was performed by CardioNerds Intern student Dr. Diane Masket.
If you haven’t already, be sure to check out CardioNerds episode #350 where we discuss the basics and mechanism of action of GLP-1 RAs with Dr. Dennis Bruemmer.
This episode was produced in collaboration with the American Society of Preventive Cardiology (ASPC) with independent medical education grant support from Novo Nordisk. See below for continuing medical education credit.
Claim CME for this episode HERE.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Prevention Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
For which patients are GLP-1 RAs recommended to reduce the risk of major cardiac events?
Can we still prescribe GLP-1 Ras in patients with well-controlled T2DM?
Is there evidence to suggest oral vs injectable GLP-1 RAs with respect to cardiac outcomes?
What side effects can patients expect when initiating GLP-1 RAs?
What does the literature say regarding the combined use of SGLT2 inhibitors and GLP-1 RAs?
The following question refers to Section 13 of the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
The question is asked by Western Michigan University medical student and CardioNerds Intern Shivani Reddy, answered first by Mayo Clinic Cardiology Fellow and CardioNerds Academy Faculty Dr. Dinu Balanescu, and then by expert faculty Dr. Harriette Van Spall.
Dr. Van Spall is an Associate Professor of Medicine, cardiologist, and Director of E-Health at McMaster University. Dr Van Spall is a Canadian Institutes of Health Research-funded clinical trialist and researcher with a focus on heart failure, health services, and health disparities.
The Decipher the Guidelines: 2022 AHA / ACC / HFSA Guideline for The Management of Heart Failure series was developed by the CardioNerds and created in collaboration with the American Heart Association and the Heart Failure Society of America. It was created by 30 trainees spanning college through advanced fellowship under the leadership of CardioNerds Cofounders Dr. Amit Goyal and Dr. Dan Ambinder, with mentorship from Dr. Anu Lala, Dr. Robert Mentz, and Dr. Nancy Sweitzer. We thank Dr. Judy Bezanson and Dr. Elliott Antman for tremendous guidance.
Palliative and supportive care has a role for patients with heart failure only in the end stages of their disease.
TRUE
FALSE
Explanation
The correct answer is False
Palliative care is patient- and family-centered care that optimizes health-related quality of life by anticipating, preventing, and treating suffering and should be integrated into the management of all stages of heart failure throughout the course of illness. The wholistic model of palliative care includes high-quality communication, estimation of prognosis, anticipatory guidance, addressing uncertainty, shared decision-making about medically reasonable treatment options, advance care planning; attention to physical, emotional, spiritual, and psychological distress; relief of suffering; and inclusion of family caregivers in patient care and attention to their needs during bereavement.
As such, for all patients with HF, palliative and supportive care—including high-quality communication, conveyance of prognosis, clarifying goals of care, shared decision-making, symptom management, and caregiver support—should be provided to improve QOL and relieve suffering (Class 1, LOE C-LD).
For conveyance of prognosis, objective risk models can be incorporated along with discussion of uncertainty since patients may overestimate survival and the benefits of specific treatments – “hope for the best, plan for the worst.”
For clarifying goals of care, the exploration of each patient’s values and concerns through shared decision-making is essential in important management decisions such as when to discontinue treatments, when to initiate palliative treatments that may hasten death but provide symptom management, planning the location of death, and the incorporation of home services or hospice.
It is a Class I indication that for patients with HF being considered for, or treated with life-extending therapies, the option for discontinuation should be anticipated and discussed through the continuum of care, including at the time of initiation, and reassessed with changing medical conditions and shifting goals of care (LOE C-LD).
Caregiver support should also be offered to family members even beyond death to help them cope with the grieving process.
A formal palliative care consult is not needed for each patient, but the primary team should exercise the above domains to improve processes of care and patient outcomes.
Specialist palliative care consultation can be useful to improve QOL and relieve suffering for patients with heart failure—particularly those with stage D HF who are being evaluated for advanced therapies, patients requiring inotropic support or temporary mechanical support, patients experiencing uncontrolled symptoms, major medical decisions, or multimorbidity, frailty, and cognitive impairment (Class 2a, LOE B). Studies have been mixed on if the palliative team itself improves quality of life and well-being so these interventions should be tailored to each patient and caregiver.
For patients with HF, execution of advanced directives can be useful to improve documentation of treatment preferences, delivery of patient-centered care, and dying in a preferred place (Class 2a, LOE C-LD).
In patients with advanced HF with expected survival < 6 months, timely referral to hospice can be useful to improve QOL (Class 2a, LOE C-LD)
Main Takeaway
In summary, the core principles of palliative care that include communication, transparency on prognosis, clarification of goals of care, shared decision-making, symptom management, and caregiver support should be integrated into each patient’s treatment plan regardless of the stage of heart failure
Guideline Loc.
Section 13, Figure 15, Table 32
Decipher the Guidelines: 2022 Heart Failure Guidelines Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
CardioNerds cofounder Dr. Dan Ambinder joins Dr. Angie Molina, Dr. Cullen Soares, and Dr. Andrew Lutz from the University of Maryland Medical Center for some beers and history by Fort McHenry. They discuss a case of disseminated haemophilus influenza
presumed fulminant bacterial myocarditis with mixed septic/cardiogenic shock. Expert commentary is provided by Dr. Stanley Liu (Assistant Professor, Division of Cardiovascular Medicine, University of Maryland School of Medicine). Episode audio was edited by Dr. Chelsea Amo-Tweneboah.
A woman in her twenties with a history of intravenous drug use presented with acute onset fevers and sore throat, subsequently developed respiratory distress and cardiac arrest, and was noted to have epiglottic edema on intubation. She developed shock and multiorgan failure. ECG showed diffuse ST elevations, TTE revealed biventricular dysfunction, and pleural fluid culture grew Haemophilus influenza. Right heart catheterization showed evidence of cardiogenic shock. She improved with supportive care and antibiotics.
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” – Sir William Osler. CardioNerds thank the patients and their loved ones whose stories teach us the Art of Medicine and support our Mission to Democratize Cardiovascular Medicine.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Case Reports Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
CardioNerds Dr. Rick Ferraro (CardioNerds Academy House Faculty and Cardiology Fellow at JHH), Dr. Gurleen Kaur (Director of the CardioNerds Internship and Internal Medicine resident at BWH), and Dr. Alli Bigeh (Cardiology Fellow at the Ohio State) as they discuss the growing obesity epidemic and how it relates to cardiovascular disease with Dr. Ambarish Pandey (Cardiologist at UT Southwestern Medical Center). Show notes were drafted by Dr. Alli Bigeh. CardioNerds Academy Intern and student Dr. Shivani Reddy performed audio editing.
Obesity is an important modifiable risk factor for cardiovascular disease, and it is on the rise! Here, we discuss how to identify patients with obesity and develop an approach to address current lifestyle recommendations. We also discuss the spectrum of pharmacologic treatment options available, management strategies, and some therapy options that are on the horizon.
This episode was produced in collaboration with the American Society of Preventive Cardiology (ASPC) with independent medical education grant support from Novo Nordisk. See below for continuing medical education credit.
Claim CME for this episode HERE.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.
CardioNerds Prevention Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
How do we identify and define obesity?
What are some current lifestyle recommendations for obese patients?
What are some tips for addressing lifestyle modifications with patients?
What are the current pharmacologic options for weight loss? Which are the most effective?
Compare and contrast the GLP-1 agents, specifically semaglutide and liraglutide.
What other newer agents are on the horizon for treatment of obesity?
Discuss some strategies to mitigate the GI side effects when using GLP-1 receptor agonists.
CardioNerds join Dr. Ethan Fraser and Dr. Austin Culver from the MedStar Georgetown University Hospital internal medicine and cardiology programs in our nation’s capital. They discuss the following case involving an unusual case of rapidly progressive heart failure. Episode audio was edited by CardioNerds Academy Intern and student Dr. Pacey Wetstein. Expert commentary was provided by advanced heart failure cardiologist Dr. Richa Gupta.
A 55-year-old male comes to the clinic (and eventually into the hospital) for what appears to be a straightforward decompensation of his underlying cardiac disease. However, things aren’t as simple as they might appear. In this episode, we will discuss the outpatient workup for non-ischemic cardiomyopathy and discuss the clinical indicators that we as clinicians should be aware of in these sick patients. Furthermore, we will discuss the differential for NICM, the management of patients with this rare disease, and how this disease can mimic other cardiomyopathies.
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.” – Sir William Osler. CardioNerds thank the patients and their loved ones whose stories teach us the Art of Medicine and support our Mission to Democratize Cardiovascular Medicine.
US Cardiology Review is now the official journal of CardioNerds! Submit your manuscript here.

CardioNerds Case Reports Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
1. What is Giant Cell Myocarditis?
Giant cell myocarditis is a rare and rapidly progressive cause of heart failure due to T-cell lymphocyte mediated myocardial inflammation. The pathogenesis of GCM is incompletely understood – histologically, there is infiltration of the myocardium by T-lymphocytes and macrophages, and there is typically evidence of upregulation of IL-17 and TNF-a. Classically, the disease state is associated with electrical (e.g., ventricular tachycardia, high-grade AV block) and hemodynamic instability – all of which typically progresses rapidly over a period of weeks to months. This male-predominant disease tends to occur in young and middle-aged patients – with a mean age between 42 and 60 based on several registries. While a rare disease, a high index of suspicion is necessary when patients present with rapidly progressive or fulminant heart failure, as a missed diagnosis of giant cell myocarditis is invariably fatal. Early and rapid identification of this uniquely high-risk group of heart failure patients and prompt initiation of therapy targeted towards the underlying autoimmune process, as well as management at a center with advanced heart failure and cardiovascular ICU support, is necessary.
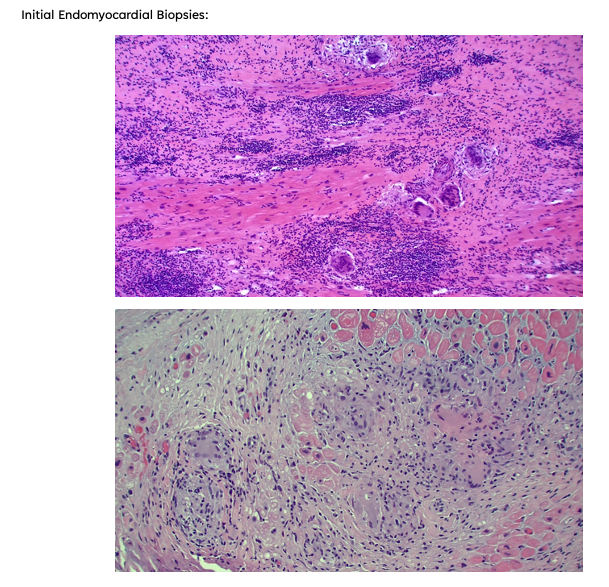
2. How is Giant Cell Myocarditis Diagnosed?
Establishing a diagnosis requires an endomyocardial biopsy (EMB), although EMB has imperfect sensitivity for GCM. Cardiac biomarkers and imaging serve an adjunct role in diagnosis; TTE findings can be variable, with either normal or dilated LV cavity size and increased wall thickness, which may be related to acute edema and inflammation. Worse LVEF on presentation has been shown to correlate with shorter transplant-free survival time. Troponin levels may be elevated, but case series have shown a lack of correlation between prognosis and troponin elevation in GCM, and importantly, in some cases, troponin values have been negative in patients later found to have GCM by biopsy. Advanced imaging is not always practical as these patients are often hemodynamically unstable, but CMR can demonstrate findings typical of myocarditis (i.e. the 2018 Lake Louise criteria).
3. What is the treatment for Giant Cell Myocarditis, and what are the future steps for disease management?
Cyclosporine-based combination immunosuppressive therapy, in addition to standard heart failure guideline-directed medical and procedural therapy and management of arrhythmias, can improve outcomes in these patients. Typical regimens include cyclosporine, high-dose steroids as the mainstay, and azathioprine or alemtuzumab (an anti-CD52 monoclonal antibody) as adjunctive agents. Patients are often co-managed by advanced heart failure, cardiac intensivists, and rheumatology. As the disease progresses, patients often develop sustained or symptomatic ventricular tachycardia, conduction abnormalities refractory HF with a dilated LV phenotype and many require mechanical circulatory support and/or cardiac transplantation.
GCM can remit and relapse, sometimes many years after initial diagnosis; an advanced heart failure team should follow these patients and should continue some immunosuppression (usually a calcineurin inhibitor) for at least 2 years. Overall, our understanding of the mechanism and management of GCM continues to evolve; high-grade evidence such as randomized controlled trials are extremely difficult to perform due to the rarity and high acuity of these presentations, therefore enrolling these patients in shared multicenter registries where able is essential to shrinking our knowledge gaps of this rare disease state.
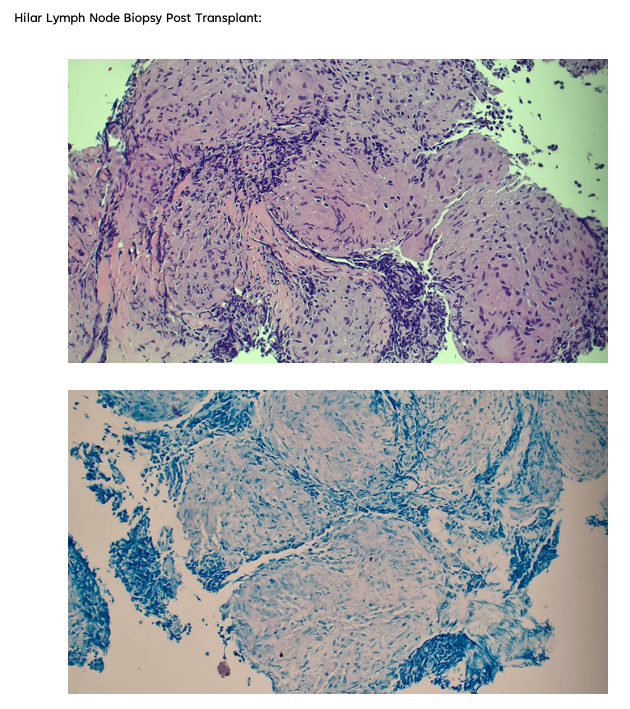
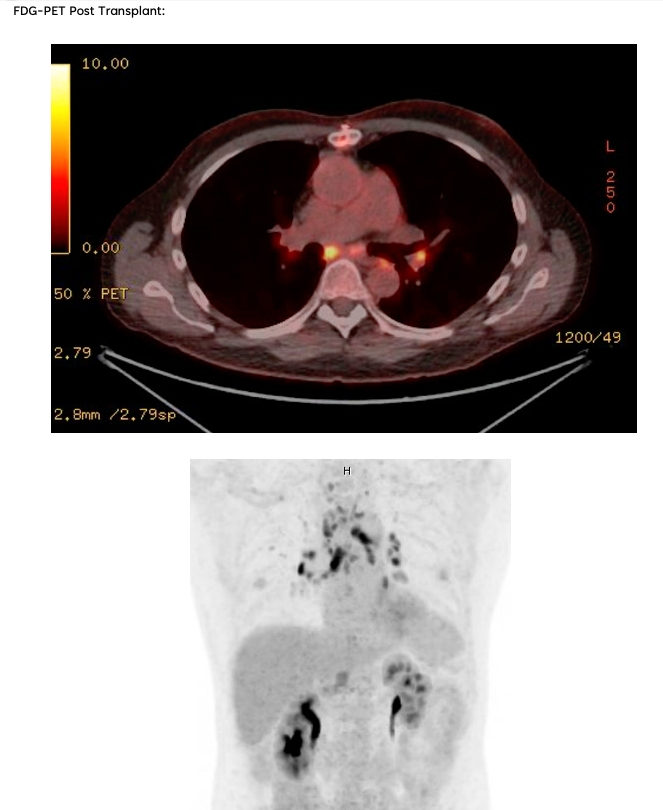
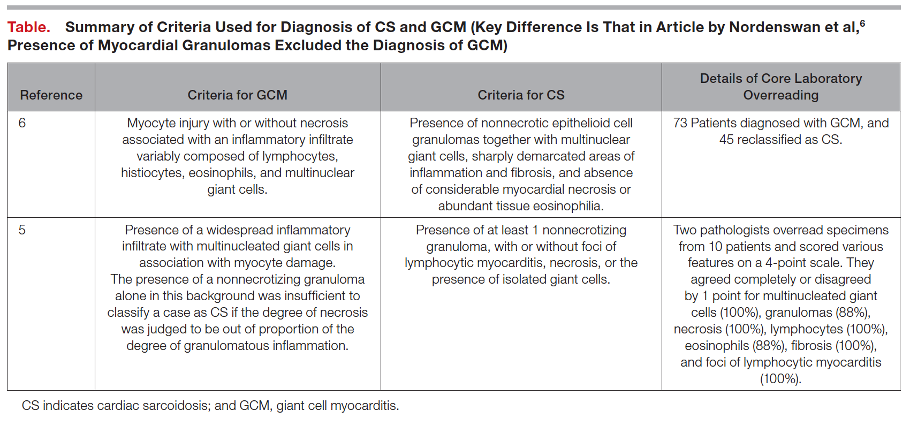
4. What else should one consider in presumed cases of Giant Cell Myocarditis?
There exists a significant clinical overlap between Giant Cell Myocarditis and Cardiac Sarcoidosis, so much so that some argue the two diseases exist on opposite ends of one disease spectrum. Both notably present with significant arrhythmia burden and advanced heart failure symptoms, although they are both treated quite differently and present with different time courses (mean time to onset of symptoms 0.3 months for GCM, 7 months for CS). Furthermore, data from Nordenswan et al. from Finland reveals that the diagnosis of GCM on histology was recategorized to CS in 62% of their studies reviewed upon secondary pathology review. To this end, it is important that clinicians consider further advanced imaging modalities (i.e., FDG-PET) in equivocal cases and consider expert pathology evaluation of endomyocardial biopsy samples as proper escalation of care and rapid identification can prevent significant treatment delays.
The following question refers to Section 9.5 of the 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure.
The question is asked by Keck School of Medicine USC medical student & former CardioNerds Intern Hirsh Elhence, answered first by Vanderbilt Cardiology Fellow and CardioNerds Academy Faculty Dr. Breana Hansen, and then by expert faculty Dr. Javed Butler.
Dr. Butler is an advanced heart failure and transplant cardiologist, President of the Baylor Scott and White Research Institute, Senior Vice President for the Baylor Scott and White Health, and Distinguished Professor of Medicine at the University of Mississippi
The Decipher the Guidelines: 2022 AHA / ACC / HFSA Guideline for The Management of Heart Failure series was developed by the CardioNerds and created in collaboration with the American Heart Association and the Heart Failure Society of America. It was created by 30 trainees spanning college through advanced fellowship under the leadership of CardioNerds Cofounders Dr. Amit Goyal and Dr. Dan Ambinder, with mentorship from Dr. Anu Lala, Dr. Robert Mentz, and Dr. Nancy Sweitzer. We thank Dr. Judy Bezanson and Dr. Elliott Antman for tremendous guidance.
Mrs. Hart is a 70-year-old woman who was admitted to the CICU two days ago for signs and symptoms consistent with cardiogenic shock. Since her admission, she has been on maximal diuretics, requiring greater doses of intravenous dobutamine. Unfortunately, her liver and renal function continue to worsen, and urine output is decreasing. A right heart catheterization reveals elevated biventricular filling pressures with a cardiac index of 1.7 L/min/m2 by the Fick method.
What is the next best step?
A
Continue current measures and monitor for improvement
B
Switch from dobutamine to norepinephrine
C
Place an intra-aortic balloon pump (IABP)
D
Resume guideline directed medical therapy
Explanation
The Correct answer is C – Place an intra-aortic balloon pump.
This patient is between the SCAI Shock Stages C and D with elevated venous pressures, decreased urine output, and worsening signs of hypoperfusion. She has been started on appropriate therapies, including diuresis and inotropic support. The relevant Class 2a recommendation is that in patients with cardiogenic shock, temporary MCS is reasonable when end-organ function cannot be maintained by pharmacologic means to support cardiac function (LOE B-NR). Thus, the next best step is a form of temporary MCS. IABP is appropriate to help increase coronary perfusion and offload the left ventricle. In fact, for patients who are not rapidly responding to initial shock measures, triage to centers that can provide temporary MCS may be considered to optimize management (Class 2b, LOE C-LD).
The guidelines further state that in patients presenting with cardiogenic shock, placement of a pulmonary arterial line may be considered to define hemodynamic subsets and appropriate management strategies (Class 2B, LOE B-NR). And so, if time allows escalation to MCS should be guided by invasively obtained hemodynamic data via PA catheterization. Several observational experiences have associated PA catheterization use with improved outcomes, particularly in conjunction with short-term MCS. Additionally, PA catheterization is useful when there is diagnostic uncertainty as to the cause of hypotension or end-organ dysfunction, particularly when the patient in shock is not responding to empiric initial measures, such as in this patient.
There are additional appropriate measures at this time that are more institution-dependent. An institutional shock team would be very helpful here as they often comprise multidisciplinary teams of heart failure and critical care specialists, interventional cardiologists, surgeons, and palliative care specialists. As such, there is a Class 2a recommendation that in patients with cardiogenic shock, management by a multidisciplinary team experienced in shock is reasonable (LOE B-NR). Most documented experiences have suggested outcomes improve after shock teams are instituted. For instance, in one such experience, using a shock team was associated with improved 30-day all-cause mortality (HR, 0.61; 95% CI, 0.41–0.93) and reduced in-hospital mortality (61.0% vs. 47.9%; P=0.041).
Choice A – Continue current measures and monitor for improvement – is incorrect. This patient has been deteriorating on current measures since admission and is at higher risk for SCAI Shock Stage E – extremis, refractory hypotension/hypoperfusion, and cardiac arrest and, therefore requires escalation of therapy
Choice B- Switch from dobutamine to norepinephrine – is incorrect. The Class 1 LOE B-NR recommendation is that in patients with cardiogenic shock, intravenous inotropic support should be used to maintain systemic perfusion and maintain end-organ performance. Dobutamine is a more potent inotropic agent than norepinephrine. Stopping dobutamine in the setting of her low cardiac index would be incorrect.
Choice D – Resume guideline-directed medical therapy – is incorrect. This patient’s shock is getting worse. The Class 1 LOE B-NR recommendation is that in patients with HFrEF, GDMT should be initiated during hospitalization after clinical stability is achieved. Restarting medications now would be premature.
Main Takeaway
In patients with cardiogenic shock, temporary MCS is reasonable when end-organ function cannot be maintained by pharmacologic means to support cardiac function.
Guideline Loc.
Section 9.5
Decipher the Guidelines: 2022 Heart Failure Guidelines Page
CardioNerds Episode Page
CardioNerds Academy
Cardionerds Healy Honor Roll
CardioNerds Journal Club
Subscribe to The Heartbeat Newsletter!
Check out CardioNerds SWAG!
Become a CardioNerds Patron!
Your feedback is valuable to us. Should you encounter any bugs, glitches, lack of functionality or other problems, please email us on [email protected] or join Moon.FM Telegram Group where you can talk directly to the dev team who are happy to answer any queries.
 The Curbsiders Internal Medicine Podcast
The Curbsiders Internal Medicine Podcast
 Eagle's Eye View: Your Weekly CV Update From ACC.org
Eagle's Eye View: Your Weekly CV Update From ACC.org
 Core IM | Internal Medicine Podcast
Core IM | Internal Medicine Podcast
 The Clinical Problem Solvers
The Clinical Problem Solvers
 JACC Podcast
JACC Podcast
 This Week in Cardiology
This Week in Cardiology