🚀 From Google Podcasts to Moon FM in No Time: Your Hassle-Free Migration Guide
👉

Rational Evidence Based Evaluation of Literature

 Take Home Points
Take Home Points
Click here for Direct Download of the Podcast.
Definition:
Epidemiology: (Anon 2004)
Presentation:
Classification of Sinusitis:
●Acute viral rhinosinusitis (AVRS)
●Uncomplicated acute bacterial rhinosinusitis (ABRS)
●Complicated acute bacterial rhinosinusitis
Sinusitis: Viral vs. Bacterial:
The Data Behind Antibiotic Use
IDSA Recommendations for Antibiotic Treatment (Chow 2012)
Bottom Line: Given the risk for adverse events associated with antibiotic use, the growing specter of resistance and the lack of significant differences in outcomes with antibiotic use, it is better to avoid antibiotics in most patients with ARS. Antibiotics should be considered in those with severe disease and in immunocompromised patients
Take Home Points
References
Read More
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 121.0 – Acute Sinusitis appeared first on REBEL EM - Emergency Medicine Blog.

Podcast Direct Download: Link
Release Date: April 16th, 2024
Show Notes
Dr. Glaucomflecken: Power of Ultrasound with Emergency Medicine Dr. Resa Lewiss
Adaira I Landry MD
Resa E Lewiss MD is a Professor of Emergency Medicine at the University of Alabama at Birmingham. A TEDMED speaker and TimesUp Healthcare founder, she’s an internationally renowned point-of-care ultrasound educator and champion for diverse, equitable, and inclusive workplaces. She attended college at Brown, medical school at Penn, Emergency Medicine residency at Harvard, and fellowship at Mount Sinai St. Luke’s Roosevelt. She led point-of-care ultrasound sections at St. Luke’s Roosevelt, the University of Colorado, and Thomas Jefferson. A physician healthcare design consultant for Perkins&Will, her design focus has been ultrasound hardware and workflows. She’s helped to redesign the built environment of a Harvard ICU and an infectious diseases unit in Malawi. As host and founder of the Visible Voices Podcast, she’s interviewed dozens of subject matter experts in healthcare, equity, and current trends. Her writings are published in the popular press and scientific journals, such as Harvard Business Review, Slate, Nature, and Fast Company. Her new book, MicroSkills : Small Actions, Big Impact is forthcoming from HarperCollins in 2024.
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL EM Book Club – MicroSkills appeared first on REBEL EM - Emergency Medicine Blog.

Click here for Direct Download of the Podcast.
Dr. Dara Kass is a practicing emergency medicine physician who was most recently as the Regional Director of Region 2 for the US Department of Health and Human Services.
She currently works with organizations and institutions to advance and implement policies that affect the care of individuals in this new healthcare landscape, most specially related to all forms of reproductive health care from contraception and pregnancy termination to addressing the maternal mortality crisis in the United States.. Doctor Kass’s impact is broad as a tireless advocate, spearheading initiatives, and campaigns formatting improvements on issues such as gender equity, reproductive healthcare, and organ donation. Doctor Kass lives in Scarsdale NY with her husband and three children.
Dr. Monica Saxena is a practicing emergency physician and assistant professor at Stanford University School of Medicine.
Her research focuses on reproductive justice and women’s health in the emergency department setting. Dr. Saxena is the 2022 recipient of the Rising Star Faculty Award from the American College of Emergency Physicians. She holds a law degree from the University of Michigan and a medical degree from Wayne State University School of Medicine.
MedPage Today: The Ethos of Emergency Medicine Hangs in the Balance
Resources:
Reproductiverights.gov
Submit your complaint to the State Survey Agency in the state where the hospital is located.
The post REBEL Cast – EMTALA + Reproductive Health Rights appeared first on REBEL EM - Emergency Medicine Blog.

 Background: The mainstay of treatment for symptomatic pulmonary embolism (PE) is anticoagulation (AC). Patients with higher-risk PE may require advanced interventions such as thrombolytic therapy, surgical thrombectomy, or even extracorporeal membrane oxygenation (ECMO). Because of its short half-life and availability of a reversal agent, unfractionated heparin (UFH) is commonly used when percutaneous or surgical interventions are being considered.
Background: The mainstay of treatment for symptomatic pulmonary embolism (PE) is anticoagulation (AC). Patients with higher-risk PE may require advanced interventions such as thrombolytic therapy, surgical thrombectomy, or even extracorporeal membrane oxygenation (ECMO). Because of its short half-life and availability of a reversal agent, unfractionated heparin (UFH) is commonly used when percutaneous or surgical interventions are being considered.
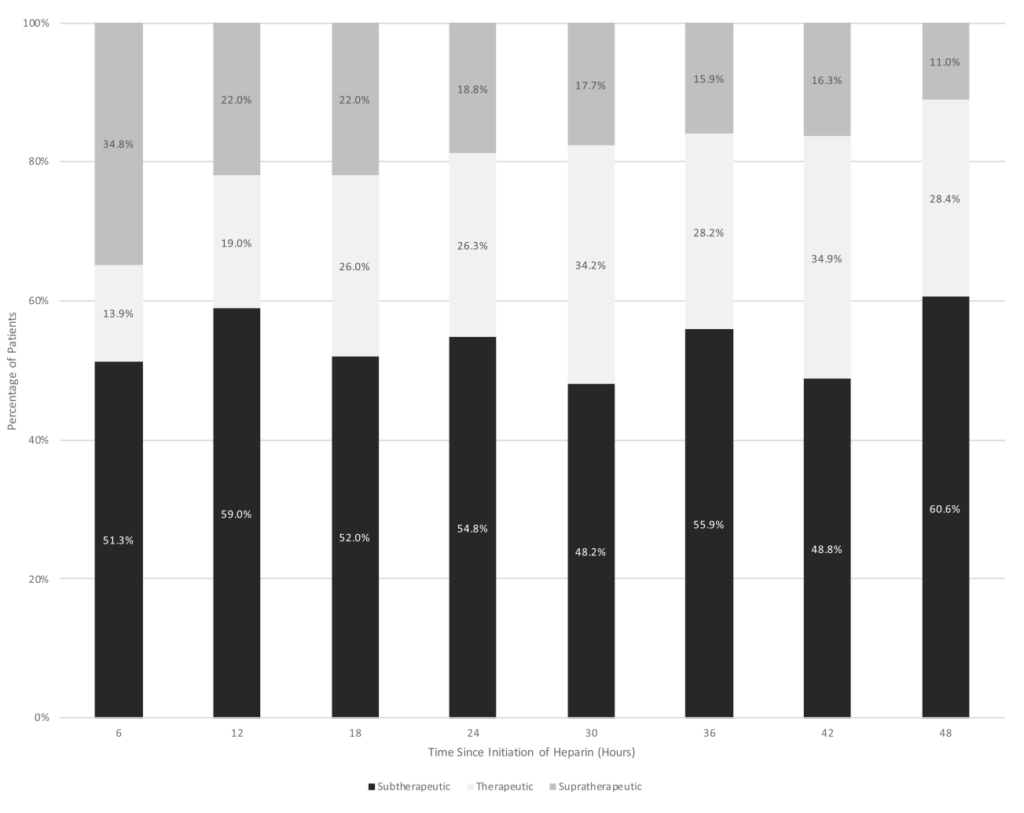
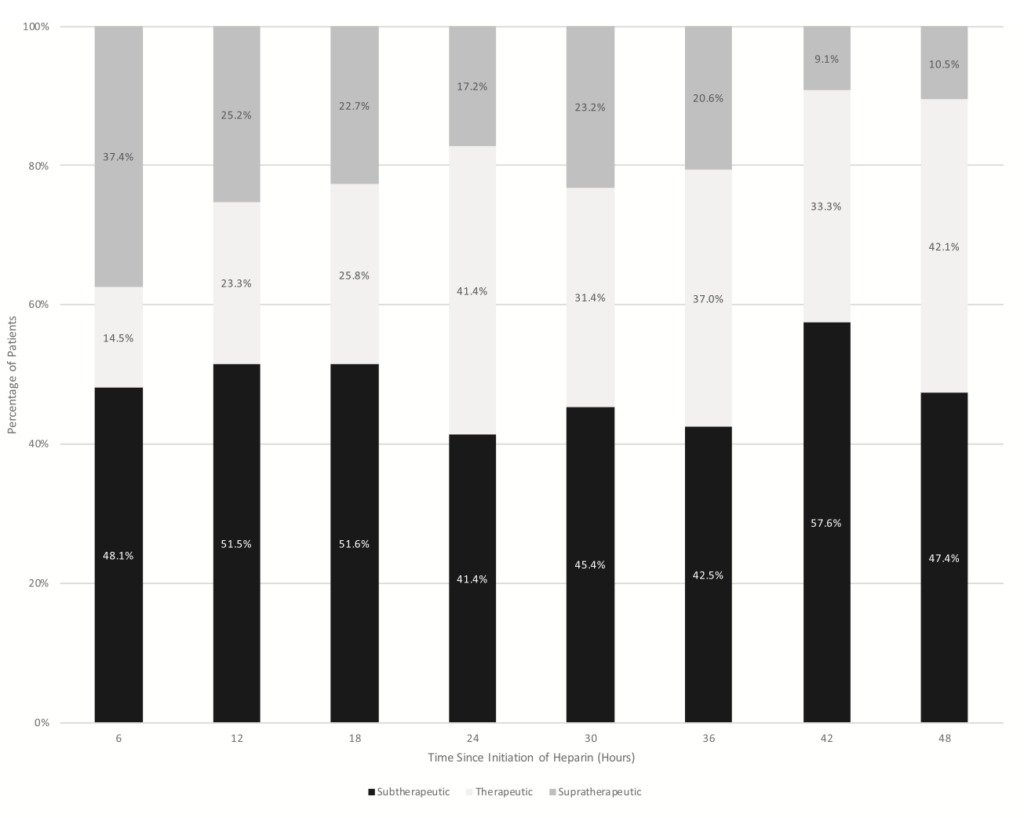
The standard weight based dosing of UFH is 80U/kg bolus followed by an infusion started at 18U/kg/hr, titrated to a target activated partial thromboplastin time (aPTT) of 1.5 to 2.5x the control range or an anti-Xa level of 0.3 to 0.7u/mL. The efficacy of UFH in reaching and maintaining appropriate anticoagulation is poorly understood.
Click here for Direct Download of the Podcast
Paper: Prucnal CK et al. Analysis of Partial Thromboplastin Times in Patients With Pulmonary Embolism During the First 48 Hours of Anticoagulation With Unfractionated Heparin. Acad Emerg Med 2020. PMID: 31625654
Clinical Question: How effective is UFH in obtaining appropriate anticoagulation during the first 48 hours of administration to patients with acute PE?
What They Did:
Outcomes:
Inclusion:
Exclusion:
Results:
Strengths:
Limitations:
Discussion:
Author Conclusion: “The majority of patients with acute PE spend most of their first 48 hours outside of the therapeutic range of AC when treated with guideline standard dosing of UFH. Over half of the patients fail to achieve any therapeutic PTT level within 24 hours of UFH initiation, and no patient had all therapeutic aPTTs. Future research should focus on identifying factors associated with achieving therapeutic AC with UFH.”
Clinical Take Home Point: In this single center study of PERT team consulted PE patients standard dosing of UFH left most patients with a subtherapeutic aPTT level in the first 48 hours of treatment. Either we need to question the dosing regimen we use for UFH or we should consider switching to LMWH in the initial treatment of PE patients.
References:
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter/X: @EMSwami)
The post REBEL Cast Ep125: 1st 48 Hours of PE Management – How Good Is Unfractionated Heparin? appeared first on REBEL EM - Emergency Medicine Blog.

 Background: Nitrates can help improve symptoms and ischemia in the setting of acute myocardial infarction. Current teaching holds that nitrates should be avoided in patients with potential right ventricular myocardial infarction (RVMI), due to the risk of decreasing preload and precipitating hypotension. This belief is based on a single 1989 study of 40 patients with RVMI and endorsed by both the AHA and ESC guidelines [2].
Background: Nitrates can help improve symptoms and ischemia in the setting of acute myocardial infarction. Current teaching holds that nitrates should be avoided in patients with potential right ventricular myocardial infarction (RVMI), due to the risk of decreasing preload and precipitating hypotension. This belief is based on a single 1989 study of 40 patients with RVMI and endorsed by both the AHA and ESC guidelines [2].
In that 1989 study, of the 40 patients with RV infarction 20 had a decrease in blood pressure of ≥30mmHg and associated symptoms after the administration of nitrates (SL, Oral, Transdermal, or IV) and 20 did not. The conclusion of this paper was that inferior AMI with RV involvement has a strong association with hypotensive response to nitrates. The major issue is the study is limited by the fact that we are given no information on dosage and multiple routes of administration making clinical application difficult. Better data is needed to guide management.
Click here for Direct Download of the Podcast
Paper: Wilkinson-Stokes M et al. Adverse Events From Nitrate Administration During Right Ventricular Myocardial Infarction: A Systematic Review and Meta-Analysis. Emerg Med J 2023. PMID: 36180168
Clinical Question: Is giving nitrates to patients with right ventricular myocardial infarction (RVMI) associated with increased adverse events compared with nitrate administration to patients with myocardial infarctions in other regions of the heart?
What They Did:
Outcomes:
Inclusion:
Exclusion:
Results:
Strengths:
Limitations:
Discussion:
Author Conclusion: “This review suggests that the AHA and ESC contraindications are not supported by evidence. Key limitations include all studies having concomitant inferior and RVMI, not evaluating beneficial effects and very low certainty of evidence. As adverse events are transient and easily managed, nitrates are a reasonable treatment modality to consider during RVMI on current evidence.”
Clinical Take Home Point: From a clinical perspective, the potential benefit of analgesia and reduced sympathetic stimulation in the setting of RVMI seems to outweigh the potential of transient hypotension with the use of nitrates. Although better studies are needed, this systematic review and meta-analysis argues against a contraindication against nitrates in the setting of RVMI and maybe one of precaution.
References:
For More Thoughts on This Topic Checkout:
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter/X: @EMSwami)
The post REBEL Cast Ep124: Nitrates in Right Sided MIs? appeared first on REBEL EM - Emergency Medicine Blog.

Click here for Direct Download of the Podcast
Employ sleep strategies:
Melatonin timing/dosing:
Caffeine:
Diet:
Don’t drive sleepy:
References
Sleep strategies:
Melatonin
Caffeine
Diet
Driving Sleepy
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 119.0 – Sleep Hygiene appeared first on REBEL EM - Emergency Medicine Blog.

Click here for Direct Download of the Podcast
Bottom Line Up Top: There is no difference in analgesic efficacy between oral and intramuscular NSAIDs.
Clinical Scenario: A 34-year-old woman presents to the ED with back pain. After your history and physical, you conclude that the patient’s pain is muscular in origin and likely secondary to heavy lifting while moving apartments. You contemplate analgesic options and decide that a NSAID makes sense. Should you give her PO ibuprofen or IM ketorolac?
What Your Gut Says: Give the ketorolac IM. IM ketorolac will provide better pain relief and the patient will be happier with her care since she got an ‘injection’ and, after all, she did come all the way to the hospital.
What The Evidence Says: Unlike with many areas of medicine, there is ample evidence to answer this question and most of that evidence has been around for a couple of decades. Reviewing every study would be tedious and, fortunately, we’ve got a great review article on the topic. One important thing to understand is that the different NSAIDs have widely accepted equianalgesic doses; at the right dose, all NSAIDs (whether it be naproxen, ibuprofen, ketorolac or diclofenac) give equivalent pain relief (Irizarry 2021). This allows us to look at studies with the different NSAIDs and compare them to each other.
A 2007 review of the literature concluded that there was no difference in analgesia between IM ketorolac and PO ibuprofen (Arora 2007). The study included a number of high-quality research studies:
Study
Format
Comparison
Findings
Notes
Retrospective analysis of prospectively collected data.
PO Ibuprofen 800 mg vs IM ketorolac 60 mg
No difference in analgesic effect.
Ibuprofen superior secondary to cost, ease of administration + lack of pain w/ administration.
Double-blind RCT
PO Ibuprofen 800 mg vs IM ketorolac 60 mg
No difference in analgesic effect.
Similar onset of action in mild-moderate pain.
Double-blind RCT
PO Ibuprofen 800 mg vs IM ketorolac 60 mg
No difference in analgesic effect.
Double-blind RCT
PO Ibuprofen 800 mg vs IM ketorolac 60 mg
No difference in analgesic effect.
Surgical Patients
Double-blind RCT
IM diclofenac 75 mg vs PO diclofenac 100 mg
Small difference favoring IM in terms of speed to pain relief
Authors conclude PO superior due to time to prepare injection
The data looks fairly clear in terms of analgesic efficacy but, don’t some patients simply prefer to receive a shot? While this dogmatic claim is often made, the data doesn’t appear to support it.
Schwartz and colleagues performed an ingenious trial (Schwartz 2000)
Bottom Line: Just give the NSAID by mouth. IM NSAIDs may provide slightly faster time to analgesia but, IM dosing comes with the cost of injection, pain , a longer time to prepare the dose and more intensive nursing resources to administer the medication. As long as the patient’s gut works, oral NSAIDs provide similar analgesic effects to IM dosing and should be the preferred route of administration.
Bonus Pearls:
Read More
REBEL EM: The Ketorolac Analgesic Ceiling
References
Irizarry E et al. A randomized controlled trial of ibuprofen versus ketorolac versus diclofenac for acute, nonradicular low back pain. Acad Emerg Med 2021; 28(11): 1228-35. PMID: 34133820
Arora S et al. Myth: Parenteral ketorolac provides more effective analgesia than oral ibuprofen. Can J Emerg Med 2007; 9(1): 30-2. PMID: 17391598
Wright JM et al.. NSAID use and efficacy in the emergency department: single doses of oral ibuprofen versus intramuscular ketorolac. Ann Pharmacother 1994;28:309-12. PMID: 8193414
Turturro MA et a. Intramuscular ketorolac versus oral ibuprofen in acute musculoskeletal pain. Ann Emerg Med 1995;26:117-20. PMID: 7618770
Neighbor ML et al. Intramuscular ketorolac vs oral ibuprofen in emergency department patietns with acute pain. Acad Emerg Med; 1998; 5(2): 118-122 .PMID: 9492131
Mixter CG et al. Preemptive pain control in patients having laparoscopic hernia repair: a comparison of ketorolac and ibuprofen. Arch Surg 1998;133:432-7. PMID: 9565125
Qureshi I et al. Intramuscular versus oral diclofenac for acute pain in adults with acute musculoskeletal injuries presenting to the ED setting: a prospective, double-blind, double dummy, randomised controlled trial. 2019; 36: 401-6. PMID: 31217178
Schwartz NA et al. Patient’s perceptions of route of nonsteroidal anti-inflammatory drug administration and its effect on analgesia. Acad Emerg Med 2000; 7: 857-61. PMID: 10958124
Motov S et al. Comparison of intravenous ketorolac at three single-dose regimens for treating acute pain in the emergency department: a randomized controlled trial. Ann Emerg Med 2017; 70(2): 177-84. PMID: 27993418
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 118.0 – IM vs PO NSAIDs appeared first on REBEL EM - Emergency Medicine Blog.

 Take Home Points
Take Home Points
Click here for Direct Download of the Podcast
Urinary Tract Infection/Pyelonephritis
Epidemiology:
Management:
Complications:
Chorioamnionitis
Definition: Also known as intraamniotic infection. Chorioamnionitis is a bacterial infection of fetal amnion and chorion membranes.
Epidemiology:
Diagnosis:
Evaluation (Abbrescia 2003):
Management:
Complications:
Postpartum Endometritis
Definition: Generalized uterine infection
Epidemiology:
Diagnosis:
Management:
Septic Abortion
Epidemiology:
Diagnosis:
Evaluation:
Management:
References:
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 117.0 – Infections of Pregnancy appeared first on REBEL EM - Emergency Medicine Blog.

 Background: Massive pulmonary embolism defined as sustained hypotension (SBP <90mmHg) has a high mortality which is why early recognition and thrombolytic therapy is typically recommended (AHA Class IIA; ESC Class IB) [1]. However, full-dose thrombolytic therapy (Alteplase 100mg (IV) is associated with an increase in bleeding [2]. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4].
Background: Massive pulmonary embolism defined as sustained hypotension (SBP <90mmHg) has a high mortality which is why early recognition and thrombolytic therapy is typically recommended (AHA Class IIA; ESC Class IB) [1]. However, full-dose thrombolytic therapy (Alteplase 100mg (IV) is associated with an increase in bleeding [2]. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4].
Click here for Direct Download of the Podcast
Paper: Aykan AC et al. Reduced-Dose Systemic Fibrinolysis in Massive Pulmonary Embolism: A Pilot Study. Clin Exp Emerg Med 2023. PMID: 37188358
Clinical Question: What is the efficacy and safety of low-dose (25mg) prolonged administration (over 6hrs) of alteplase in patients with massive PE?
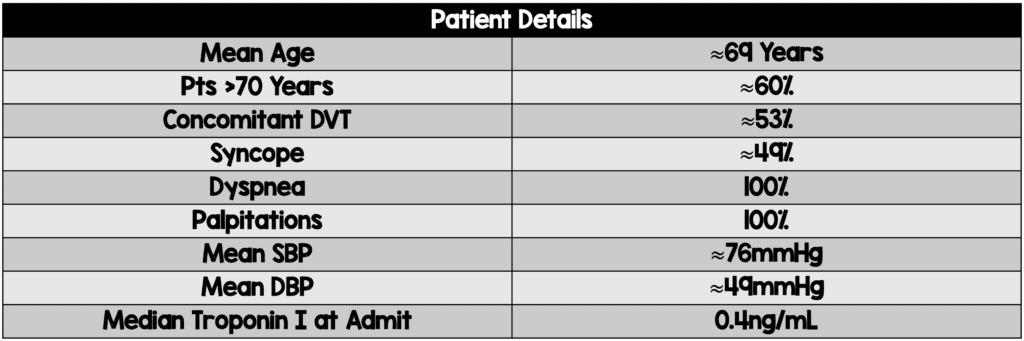
Author Conclusion: “Results of this pilot study suggest that low-dose prolonged infusion of tPA is an effective and safe therapy in patients with massive PE. This protocol was also effective in decreasing PASP and restoration of RV function.”
Clinical Take Home Point: Low dose (25mg) alteplase given as a prolonged infusion (over 6hrs) is a promising effective and safe therapy in patients with massive PE and provides an alternative to full dose (100mg) and half-dose (50mg) alteplase. Larger RCTs comparing doses of alteplase are warranted to confirm these findings.
Post Peer Reviewed By: Anand Swaminathan, MD (X: @EMSwami)
The post REBEL Cast Ep123: Reduced-Dose Systemic Peripheral Alteplase in Massive PE? appeared first on REBEL EM - Emergency Medicine Blog.

 Take Home Points
Take Home Points
Click here for Direct Download of the Podcast
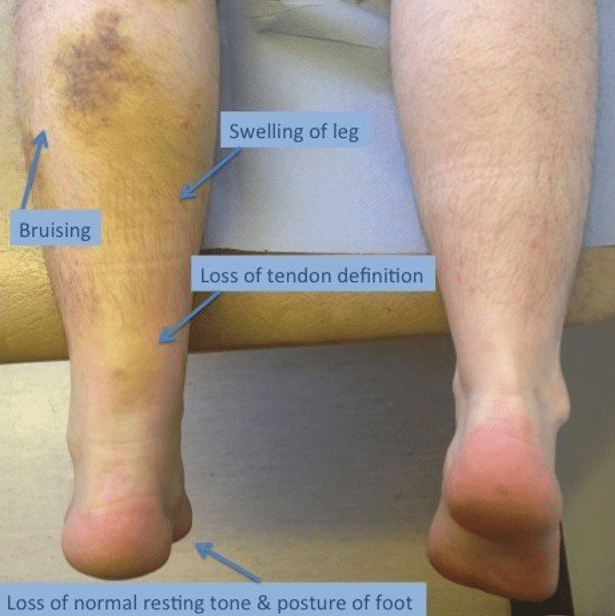 Achilles Tendon Rupture Exam (www.lfaclinic.co.uk)
Achilles Tendon Rupture Exam (www.lfaclinic.co.uk)
Physical Exam
Sensitivity
Specificity
(+) LR
(-) LR
96-100%
93-100%
13.7
0.04
Imaging
ED Management
Prognosis
Links
Orthobullets: Achilles Tendon Rupture
Resources:
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter/X: @srrezaie)
The post REBEL Core Cast 116.0 – Achilles Tendon Rupture appeared first on REBEL EM - Emergency Medicine Blog.
 Take Home Points: Know clinical (cold extremities, oliguria, confusion, dizziness, narrow pulse pressure) and laboratory markers (metabolic acidosis, elevated creatinine, lactic acidosis) of hypoperfusion. An elevated lactate is a danger sign and requires explanation. Norepinephrine is a great first line vasopressor in Cardiogenic shock. Dobutamine is useful for inotropic support in Cardiogenic shock. Use POCUS ... Read more
Take Home Points: Know clinical (cold extremities, oliguria, confusion, dizziness, narrow pulse pressure) and laboratory markers (metabolic acidosis, elevated creatinine, lactic acidosis) of hypoperfusion. An elevated lactate is a danger sign and requires explanation. Norepinephrine is a great first line vasopressor in Cardiogenic shock. Dobutamine is useful for inotropic support in Cardiogenic shock. Use POCUS ... Read more
The post REBEL Core Cast 115.0 – Cardiogenic Shock appeared first on REBEL EM - Emergency Medicine Blog.
Your feedback is valuable to us. Should you encounter any bugs, glitches, lack of functionality or other problems, please email us on [email protected] or join Moon.FM Telegram Group where you can talk directly to the dev team who are happy to answer any queries.
 EM Clerkship
EM Clerkship
 Emergency Medical Minute
Emergency Medical Minute
 The Internet Book of Critical Care Podcast
The Internet Book of Critical Care Podcast
 Critical Care Scenarios
Critical Care Scenarios
 EMCrit FOAM Feed
EMCrit FOAM Feed
 Emergency Medicine Cases
Emergency Medicine Cases